

BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://cjns.gums.ac.ir/article-1-327-en.html



2- Department of Psychology, Faculty of Literature and Humanities, University of Guilan, Rasht, Iran
3- Department of Internal Medicine and Neurology, Ghaem International Hospital, Rasht, Iran
Introduction
Multiple Sclerosis (MS) is known as a chronic and debilitating immune system disease that destroys the myelin sheath of the central nervous system (brain and spinal cord) [1, 2]. MS causes depression, anxiety, frustration, inability to perform responsibilities, impaired social functioning, and disruption of family relationships in the patients [3]. The age range for the onset of this disease is between 20 and 40 years with an average age of 30 years and its prevalence in women is two to three times more than men [4, 5]. In Iran, approximately 0.6% of the population has been reported as MS cases [6, 7].
According to the MS Association of Guilan Province, until 2015, 1376 people had been reported as MS cases. Of them, 28% were men and 72% women [8]. Over the past few decades, life quality has been recognized as an important standard for healthiness, and the World Health Organization (WHO) has defined quality of life as “people’s perception of their situations in life in the context of the culture and value systems in which they live and in response to their goals, expectations, standards, and concerns” [9].
Psychological problems in people with MS are the main source of disability, social harms, and poor quality of life. Therefore, the primary purpose of most therapies, especially in chronic diseases, is to strengthen the quality of life through the improvement of their physical and mental health and of the social life quality [10]. According to recent various research studies, patients with MS have a lower quality of life than healthy people, which can lead to incompatible inefficient coping mechanisms and tension [11-13].
On the other hand, there are some psychological symptoms, including depression, anxiety, and stress in women with MS. Humans have different types of emotional reactions, including three basic ones of sadness, fear, and anger, which manifest themselves in the form of depression, stress, and anxiety [14]. Female MS patients have more mental problems (such as depression, stress, and anxiety) than healthy ones, and experience the highest prevalence (about 48%) in the first year after the diagnosis [15]. According to studies, 50% to 60% of MS patients suffer from depression [16, 17], and between 25% and 45% of them suffer from anxiety, which severely affects their quality of life [18, 19]. In a study, Alsaadi et al. reported that the prevalence of depression in MS patients was 63.3% [20]. A study by Ackerman demonstrated a strong association between stress and the exacerbation (recurrence) of the MS disease [21].
Positive group-psychotherapy is one of the newest interventions in the field of therapy, which its clinical trial has been confirmed by various studies, including Huffman et al. (2019), Moeller et al. (2019), and Moghtaderi et al. (2020). These studies have shown that positive group psychotherapy affects psychological symptoms (depression, anxiety, stress) and improves the quality of life in a variety of individuals, indicating the effectiveness of this treatment [22-24].
As a theorist of positive psychology, Layous et al. have directly attributed the positive interventions to the wellbeing qualities and the reduction of negative emotional reactions and also have defined positive thoughts as a cause for positive behaviors and emotions [25]. In many different studies, the effect of positive psychology-based interventions on reducing psychological symptoms has been reported to be significant [26, 27]. In this regard, the studies of various researchers have shown the significant effect of positive group-psychotherapy and their components on the quality of life [28-30].
Although the effectiveness of positive interventions has been proved for healthy individuals and even for people with depression or negative emotional reactions, few studies have considered the efficacy of this approach for patients with medical conditions such as MS [27]. Therefore, regarding the importance of quality of life and the mental healthiness, and the lack of research on this field, the present study is about to answer the question of whether positive group-psychotherapy affects the psychological symptoms (depression, anxiety, and stress) and improves the quality of life of women with MS.
Materials and Methods
This quasi-experimental research has a pre-test and post-test design and a control group. The statistical population of the research included all female MS patients who had referred to the MS Association of Guilan in the summer and autumn of 2019. Sampling was performed purposefully, and 30 individuals were selected, of which 15 individuals were randomly classified as the experimental group (average age of 31.66 with a standard deviation of 8.87 years) and 15 others in the control group (Mean±SD of age was 31.60±7.693 years) (P>0.05).
The criteria for considering the individuals as the samples of the study were aged between 17 and 55 years, literate, not in the critical level of the disease, not hospitalized due to mental illness, regular participation in therapeutic sessions, and no drug addiction and without hearing or speaking issues. Any opposition to the above criteria, such as not participating in the therapeutic sessions or using other psychotherapy methods during the research, resulted in exiting from the sampling process.
The license for this study has been approved by Guilan MS Association. This study was registered by the Ethics Committee of biomedical research of Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.067 and IRCT registration number).
Measuring tools
The information in this research was gathered through the following questionnaires:
Depression Anxiety Stress Scale (DASS) questionnaire
This questionnaire was designed by Lovibond et al. (1995) and expanded by Lovibond. The questionnaire included 3 subscales (anxiety, stress, and depression) each containing 3 items. This questionnaire is rated on a 4-point Likert-type scale from 0 to 3. Its highest score in each subgroup is 21 [31]. In the Iranian population, the depression anxiety stress scale was validated by Sahebi et al. (2005) and Haji-Amini et al. (2012), and its reliability was approved by experts [32, 32]. Lovibond and Lovibond (1995) found a significant correlation between Beck’s depression inventory and depression anxiety stress scale (r=0.4) in a large statistical sample of 717 university students [31]. Moreover, Antoni et al. (1998) obtained similar patterns of correlation in clinical samples [34]. Depression anxiety stress scale is a self-assessment questionnaire scored on a 4-point Likert scale ranging from “never” to “always” [31, 32]. Internal consistency for the normative sample of this research (717 individuals) for depression subscale is r=0.81, anxiety subscale r=0.73, and stress subscale r=0.81. For scale validity, correlation coefficients or Beck anxiety and depression inventory were obtained 0.81 and 0.74 [31].
On an Iranian sample, the internal consistency of depression, anxiety, and stress scale scores were obtained using the Cronbach alpha for depression scale as 0.77, anxiety scale as 0.79, and stress scale as 0.78. The validity of the test was assessed using factor analysis (depression scale 0.61, anxiety 0.67, and stress 0.64) and criterion validity (depression 0.70, anxiety 0.67, and stress 0.49) [32].
MS Impact Scale (MSIS-29) questionnaire
Contains 29 questions; its first 20 questions measure the physical impacts, and the last 9 questions measure the psychological impacts of MS on patients. Each question contains 5 options (with a value of 1-5). The total score of the patients’ answers to these two groups of questions ranges between 0 and 100, which gives us two scales to measure the physical or psychological dimensions of life quality. The higher the score, the lower the health would be. The maximum score for the physical impact is 100, while the minimum is 20, and the maximum score for the psychological impact is 45, while its minimum is 9 [35]. The study results, regarding the validity and reliability of MSIS-29, showed that its reliability is less than 0.80 using the Cronbach alpha coefficient [36]. The convergent validity of the MSIS-29 physical subscale, using other physical inability measuring scales, indicates high correlation coefficients. For the divergent validity, the correlation between the MSIS-2 physical scale and the BDI-II depression questionnaire was 0.49. The MSIS-29 psychological subscale also had an expected high correlation with BDI-II (r=0.80). Also, for the Persian version of this questionnaire, the alpha coefficient of >0.70 and the test-retest coefficient of > 0.70 have been reported. The validity coefficient of the questionnaire was 0.71 [37].
The research sample was selected in two stages: First, 150 women with MS and members of the Guialn MS Association were selected by convenience sampling method and completed research questionnaires (DASS21 and MSIS-29). Then, based on the high scores of the questionnaires, 30 patients were selected and assigned as the experimental (intervention) and control groups.
After sampling, the whole treatment process was explained for the patients to assure them of their privacy and all of them signed the consent form. After the pretest, eight sessions of positive group psychotherapy intervention for two months were performed on the experimental group. Then, two weeks later, the post-test was performed on both groups. Then the data were analyzed using SPSS V. 23 with a univariate analysis of covariance (ANCOVA) and multivariate analysis of covariance (MANCOVA).
Procedure and duration of treatment intervention sessions
This treatment is based on a positive psychology approach designed by Rashid and Seligman (Table 1) [38].
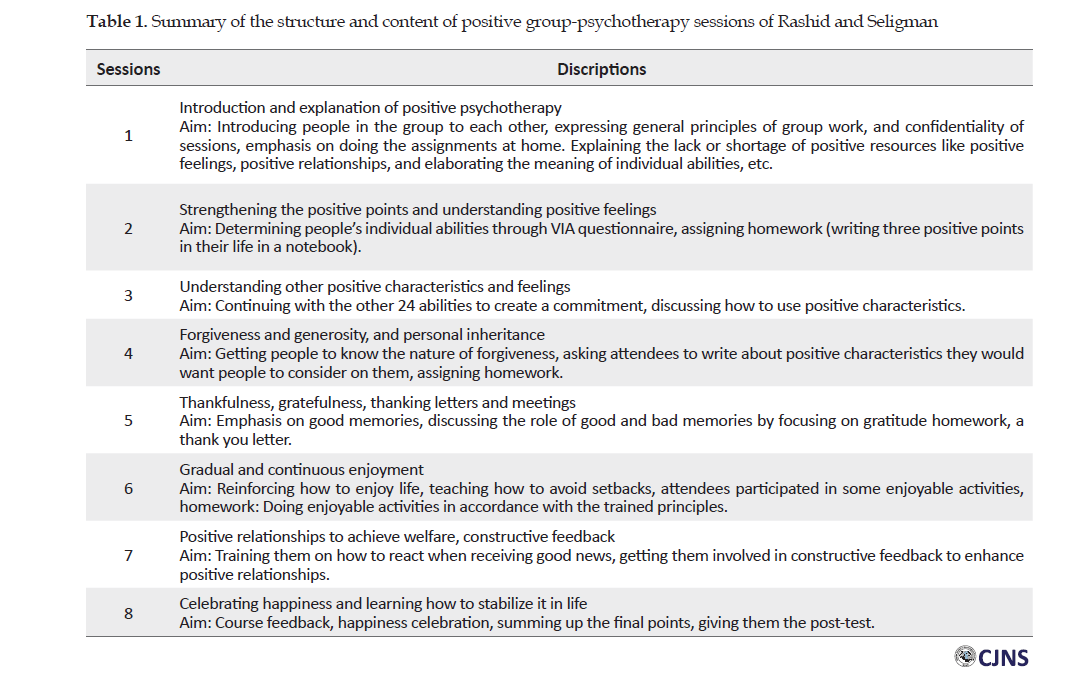
To conduct positive group psychotherapy training sessions, the author used the group form of positive psychotherapy in this study. The interventions were performed in one of the counseling centers. The treatment program was performed one day per week for 90 minutes in the fall of 2019. The treatment was performed by the first researcher of the manuscript (S.H.R) who has completed a course in positive group psychotherapy under the supervision of a tutor. As follows, the positive group-psychotherapy program training sessions will be briefly described (Table 1).
Results
To evaluate the effect of positive group-psychotherapy on the severity of depression, anxiety, stress, and quality of life in patients with MS, we used ANCOVA and MANCOVA. Before performing the analysis of covariance, the hypotheses of this statistical method were tested.
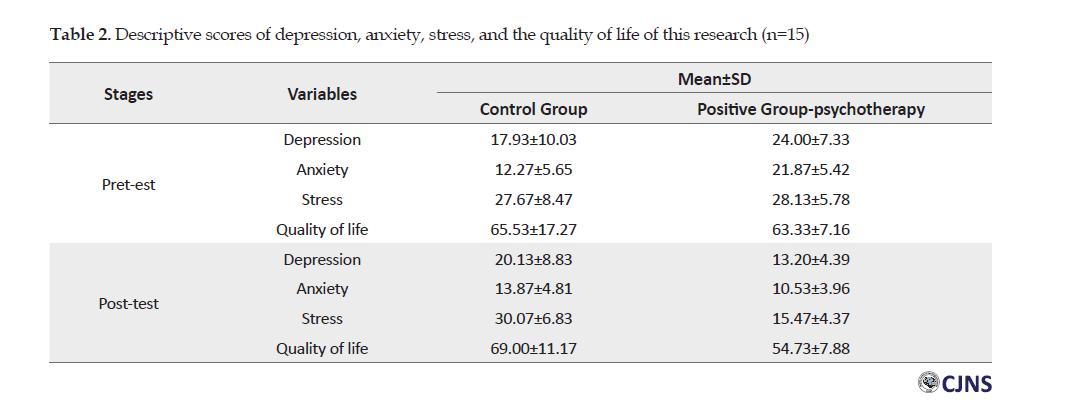
Table 2 presents the mean and standard deviation of each research variable separately for the experimental and control groups in the pre-test and post-test.
Then, the univariate output data were analyzed using a box plot diagram and the results showed no output data in the variables. In these analyses, a pre-test was considered as an auxiliary variable or covariance, and based on this, the normality of the variables, homogeneity of regression slope, linear relationship, and equality of variances of the pre-test and post-test scores in the variables were investigated. Data normality test of the Kolmogorov-Smirnov and Shapiro-Wilk test were used. The results of these tests showed that the distribution of depression, anxiety, and stress scores in the control group and intervention group were normal (P>0.12). Also, the value of M. Box statistics showed that this index was not statistically significant and the assumption of homogeneity of variance of errors was established for the data of this study (F=1.71, P>0.113). The results of the Bartlett test for examining the correlation between variables were significant, which confirmed that this assumption also holds (P<0.007). The test results showed the homogeneity of the pre-test and post-test regression slope in the experimental and control groups showed that the regression slope is established for the studied variables. After reviewing and confirming the defaults, a multivariate covariance test was performed.
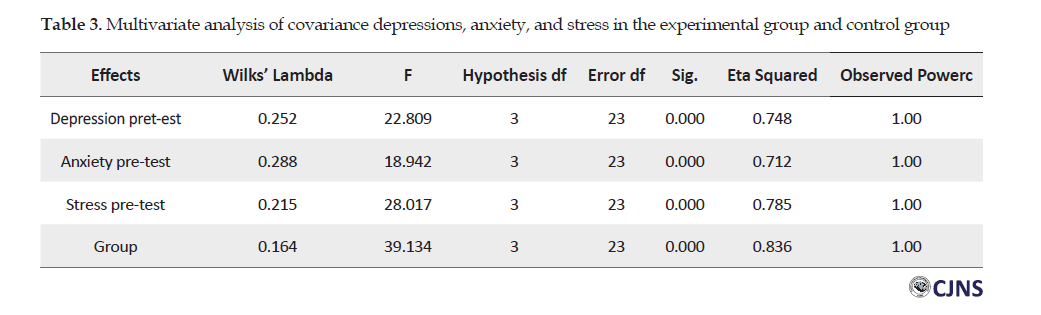
The results of the multivariate analysis of covariance showed that the differences between the groups were significant (F=39.13, P<0.001). Based on this, there is a significant difference between the control and experimental groups in the scores of depression, anxiety, and stress (Table 3).
To compare the effects of the treatment method, adjusted means (after removing the effect of pre-test) and the results of the post hoc test (pairwise comparison) with the Tukey method are reported. The results of the analysis showed a difference between the mean value of depression, anxiety, and stress in the post-test. The severity of depression (10.26), anxiety (9.66), and stress (13.02) in the experimental group (intervention group) were less than those in the control group (P<0.001).
The Kolmogorov-Smirnov and Shapiro-Wilk tests were used to extract the data and the normality test. The results of these tests showed that the distribution of quality of life scores in the control and experimental groups was normal (P>0.12). Also, the results of Levene’s test showed that the difference in variance was not significant and the assumption of homogeneity of variance was established for patients’ quality of life data (F=0.389, P>0.57). The results of the Bartlett test for examining the correlation between variables were significant, which confirms that this assumption also holds (P>0.007). The test results of the homogeneity slope of pre-test and post-test regression in the experimental and control groups showed that the regression slope is established for the quality of life. After checking and confirming the defaults, a univariate covariance test was performed. The results of the analysis of covariance showed that the differences between the groups were significant (F=50.44, P<0.001). Based on these results, there is a difference between the quality of life of the control and experimental groups (Table 4).
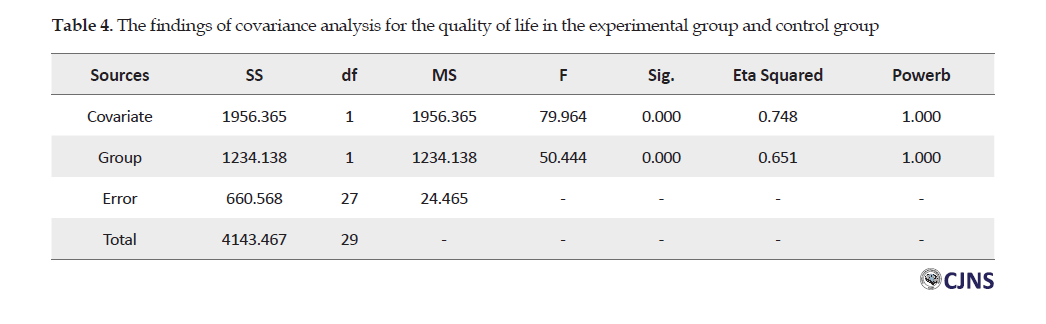
To compare the effects of the treatment method, a significant difference was reported in the scores of the adjusted means (after removing the pre-test effect) and the results of the post hoc test (pairwise comparison) with the Tukey method. Pairwise comparisons and quality of life marginal means show that the mean value in the post-test quality of life of patients in the experimental group is 12.87 points lower than that in the control group (P<0.001). In other words, the experimental group had a significant improvement in the quality of life.
Discussion
The main aim of this research was to determine the effectiveness of positive group psychotherapy on the psychological symptoms (depression, anxiety, and stress) and improving the quality of life in female patients with MS. The findings of this study showed that the positive psychotherapeutic interventional program causes a reduction in psychological symptoms (stress, anxiety, and depression) as well as improving the quality of life in women with MS. Our findings conform with positive group-psychotherapy results of studies done by Huffman et al., Moeller et al., and Moghtaderi et al. [22-24].
The first finding of this research is the effect of the positive psychotherapeutic intervention on reducing the psychological symptoms (stress, anxiety, and depression) of MS patients, which agrees with the results of authoritative research of Moghtaderi et al. and Leclaire et al. [24-27].
The psychological symptoms (stress, anxiety, and depression) in women with MS are of the most important factors that significantly reduce the patients’ mental health. Regarding the above point, the results show that positive group psychotherapy can be a way to change the thinking style of the patient, hence creating thoughts in the individual’s mind that will help him or her to cope with difficult situations, and consequently, to find appropriate solutions for problems [38]. Therefore, women with MS who have been treated by positive group-psychotherapy can rescue themselves from destructive thoughts that may cause negative psychological symptoms (stress, anxiety, and depression), so that they can replace new positive thoughts to help them better understand themselves or the world around them.
The second finding of this study is that the positive group-psychotherapy intervention can significantly improve the quality of life in female patients with MS. This finding agrees with the result of studies by Azarkolah et al. and Assarzadegan and Sadeghi et al. who studied the effectiveness of positive group-psychotherapy on improving the quality of life [28-30]. Therefore, positive group-psychotherapy reduces negative emotional reactions and increases happiness and, consequently, improves the quality of life of MS patients through increasing their positive emotions, expanding their strengths, and seeking meanings in their lives. Therefore, the more desirable the quality of life of a person, the less despair and helplessness feelings in pathological situations.
Conclusion
The results of this research showed that positive group-psychotherapy can reduce the psychological symptoms (depression, anxiety, and stress) in women with MS. Also, positive group-psychotherapy can improve the quality of life in women with MS. Furthermore, findings of this research show that feeling of being a member of a group, being supported, and experiencing positive and enjoyable events can satisfy personal needs. These factors can affect feelings of happiness, control negative emotional reactions such as depression, stress, and anxiety, and improve the quality of life of the women with MS.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by the Ethics Committee of Guilan University of Medical Sciences (No.IR.GUMS.REC.1399.067). The IRCT registration number is IRCT20200616047804N1.
Funding
This article is extracted from the PhD. thesis of Seyyed Hadi Rafieeat, at the Faculty of Department of Psychology, Ardabil Branch of Islamic Azad University (Code: 1194860396442731398162255936).
Authors contributions
Conceptualization, supervision, and writing the original draft: Somayyeh Taklavi; Investigation and methodology: Somayyeh Taklavi, Seyyed Hadi Rafiee, Abbas Abolghasemi, and Hamidreza Ghalyanchi Langroodi; Writing, review, and editing: Abbas Abolghasemi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We would like to thank Mrs. Qutbzadeh (Director of MS Guilan Association), Mrs. Fathi Moghadam (Director of Mehr-Ara Clinic), Miss. Alidastan, and other loved ones who helped us in completing this research.
References
1.Pompili M, Forte A, Palermo M, Stefani H, Lamis DA, Serafini G, et al. Suicide risk in multiple sclerosis: A systematic review of current literature. J Psychosom Res. 2012; 73(6):411-7. [DOI:10.1016/j.jpsychores.2012.09.011] [PMID]
2.Hughes N, Locock L, Ziebland S. Personal identity and the role of ‘carer’ among relatives and friends of people with multiple sclerosis. Soc Sci Med. 2013; 96:78-85. [DOI:10.1016/j.socscimed.2013.07.023] [PMID] [PMCID]
3.Ensan N, Rahimian Boogar I, Talepasand S, Estilaee F. [Effectiveness of a mindfulness-based stress reduction program on functional disability of patients with multiple sclerosis (Persian)]. J Arak Univ Med Sci. 2019; 22(5):56-67. [DOI:10.32598/JAMS.22.5.56]
4.Tauil CB, Grippe TC, Dias RM, Dias-Carneiro RPC, Carneiro NM, Aguilar ACR, et al. Suicidal ideation, anxiety, and depression in patients with multiple sclerosis. Arq Neuropsiquiatr. 2018; 76(5):296-301. [DOI:10.1590/0004-282x20180036] [PMID]
5.Foschi M, Rizzo G, Liguori R, Avoni P, Mancinelli L, Lugaresi A, et al. Sleep-related disorders and their relationship with MRI findings in multiple sclerosis. Sleep Med. 2019; 56:90-7. [DOI:10.1016/j.sleep.2019.01.010] [PMID]
6.Nasiri M, Hosseini SH, Sakhaei SY, Tabrizi N, Yazdani Cherati J, Abedini M. [Prevalence of psychiatric disorders in patients with multiple sclerosis in Mazandaran, Iran (Persian)]. J Mazandaran Univ Med Sci. 2016; 26(140):60-70. http://jmums.mazums.ac.ir/article-1-8549-en.html
7.Abdekhodaie Z, Shahidi Sh, Mazaheri MA, Panaghi L, Nejati V. [Psychological strategies to deal with illness in patients with multiple sclerosis: A phenomenological study (Persian)]. Q J Health Psychol. 2018; 6(24):7-30. http://hpj.journals.pnu.ac.ir/article_4533_en.html
8.Farhadi M, Pasandideh MM. [Mindfulness based cognitive therapy in reducing stress, anxiety, depression, and increase self-efficacy in female patients with Multiple Sclerosis (MS) (Persian)]. Clin Psychol Personal. 2018; 15(2):7-15. http://cpap.shahed.ac.ir/article-1-1152-en.html
9.Ghotbinejhad Bahre Asmani U, Ahadi H, Hatami HR, Sarami Foroushani GR. [Comparison of the effectiveness of group positive psychotherapy and group psychodrama on spiritual attitude, distress tolerance, and quality of life in women with chronic pain (Persian)]. J Anesthesiol Pain. 2019; 9(4):51-65. http://jap.iums.ac.ir/article-1-5396-en.html
10.Samin T, Akhlaghi Kohpaei H. [Prediction of life expectancy based on quality of life, perceived stress and fatigue in patients with Multiple Sclerosis (MS) (Persian)]. Q J Health Psychol. 2019; 8(29):101-18. [DOI:10.30473/HPJ.2019.38195.3857]
11.Haresabadi M, Karimi Monaghi H, Froghipor M, Mazlom SR. [Quality of life in patients with multiple sclerosis referring to Ghaem Hospital, Mashhad in 2009 (Persian)]. J North Khorasan Univ Med Sci. 2011; 2(4):7-12. [DOI:10.29252/jnkums.2.4.7]
12.Moghaddam Tabrizi F, Najarzadeh M, Raeisi FZ. [A survey on the fatigue and sleep quality and its relation with the quality of life in multiple sclerosis (Persian)]. Nurs Midwifery J. 2016; 14(1):78-87. http://unmf.umsu.ac.ir/article-1-2579-en.html
13.Rahmani S, Zeinali M, Aghaei M, Gazal S, Drodian N. [The effect of group mindfulness-based stress reduction program and conscious yoga on the quality of life and fatigue in patients with multiple Sclerosis (Persian)]. Clin Psychol Personal. 2019; 16(2):141-50. http://cpap.shahed.ac.ir/article-1-1294-en.html
14.Pekrun R, Goetz T, Titz W, Perry RP. Academic emotions in students’ self-regulated learning and achievement: A program of qualitative and quantitative research. Educ Psychol. 2002; 37(2):91-105. [DOI:10.1207/S15326985EP3702_4]
15.Mitchell AJ, Benito-León J, Morales González JM, Rivera-Navarro J. Quality of life and its assessment in multiple sclerosis: integrating physical and psychological components of wellbeing. Lancet Neurol. 2005; 4(9):556-66. [DOI:10.1016/S1474-4422(05)70166-6]
16.Blake DJ, Bodine C. An overview of assistive technology for persons with multiple sclerosis. J Rehabil Res Dev. 2002; 39(2):299-312. [PMID]
17.Besharat MA, Barati N, Lotfi J. [Relationship between coping styles and mental health in a sample of multiple sclerosis patients (Persian)]. Res Med. 2008; 32(1):27-35. http://pejouhesh.sbmu.ac.ir/article-1-457-en.html
18.Agha-Bagheri H, Mohammad-Khani P, Emrani S, Farahmand V. [The efficacy of mindfulness-based cognitive therapy group on the increase of subjective well-being and hope in patients with multiple sclerosis (Persian)]. J Clin Psychol. 2012; 4(1):23-31. [DOI:10.22075/JCP.2017.2076]
19.Saadat S, Kalantari M, Kajbaf MB, Hosseininezhad M. [A comparative study of health promoting behaviors in healthy individuals and patients with multiple sclerosis: An analytical study (Persian)]. Hayat. 2019; 25(2):138-50. http://hayat.tums.ac.ir/article-1-2944-en.html
20.Alsaadi T, El Hammasi Kh, Shahrour TM, Shakra M, Turkawi L, Mudhafar A, et al. Prevalence of depression and anxiety among patients with multiple sclerosis attending the MS clinic at Sheikh Khalifa Medical City, UAE: Cross-Sectional Study. Mult Scler Int. 2015; 2015:487159. [DOI:10.1155/2015/487159] [PMID] [PMCID]
21.Ackerman KD, Heyman R, Rabin BS, Anderson B, Houck P, Frank E, et al. Stressful life events precede exacerbations of multiple sclerosis. Psychosom Med. 2002; 64(6):916-20. [DOI:10.1097/00006842-200211000-00009] [PMID]
22.Huffman JC, Feig EH, Millstein RA, Freedman M, Healy BC, Chung WJ, et al. Usefulness of a positive psychology-motivational interviewing intervention to promote positive affect and physical activity after an acute coronary syndrome. Am J Cardiol. 2019; 123(12):1906-14. [DOI:10.1016/j.amjcard.2019.03.023] [PMID] [PMCID]
23.Moeller RW, Seehuus M. Loneliness as a mediator for college students’ social skills and experiences of depression and anxiety. J Adolesc. 2019; 73:1-13. [DOI:10.1016/j.adolescence.2019.03.006] [PMID] [PMCID]
24.Moghtaderi M, Saffarinia M, Zare H, Alipour A. [Effectiveness of the package of hope therapy based on positivist approach on the self-efficacy and loneliness of Parkinson patients (Persian)]. Q J Health Psychol. 2020; 8(32):73-92. http://hpj.journals.pnu.ac.ir/article_6498_en.html
25.Layous K, Chancellor J, Lyubomirsky S, Wang L, Murali Doraiswamy P. Delivering happiness: Translating positive psychology intervention research for treating major and minor depressive disorders. J Altern Complement Med. 2011; 17(8):675-83. [DOI:10.1089/acm.2011.0139] [PMID]
26.Rashid Almasi B, Alipour A, Elmi Manesh N. [The effect of positive psychotherapy intervention on depression, stress, and happiness infertile women (Persian)]. Semi Annu J Fam Pathol Couns Enrichment. 2019; 4(2):75-88. http://fpcej.ir/article-1-218-en.html
27.Leclaire K, Cecil A, LaRussa A, Stuart F, Hemond CC, Healy BC, et al. A pilot study of a group positive psychology intervention for patients with multiple sclerosis. Int J MS Care. 2018; 20(3):136-41. [DOI:10.7224/1537-2073.2017-002] [PMID] [PMCID]
28.Azarkolah A, Abolghasemi A, Nadrmohammadi M, Salvat H. [Determine the relationship between sense of coherence, positive thinking & self-disclosure with quality of life of cancer patients (Persian)]. Q J Health Psychol. 2020; 8(32):7-24. http://hpj.journals.pnu.ac.ir/article_6494_en.html
29.Assarzadegan M, Raeisi Z. [The effectiveness of training based on positive-psychology on quality of life and happiness of patients with type 2 diabetes (Persian)]. Q J Health Psychol. 2019; 8(30):97-116. http://hpj.journals.pnu.ac.ir/article_6039_en.html
30.Sadeghi F, Abolghasemi A, Kazemi R, Narimani M. [The effectiveness of positive cognitive-behavioral therapy on orientation of life in female teachers with chronic fatigue syndrome (Persian)]. J Clin Psychol. 2019; 11(2):23-31. https://jcp.semnan.ac.ir/index.php/article_4132_en.html
31.Lovibond SH, Lovibond PF. Manual for the depression anxiety stress scales. 2nd ed. Sydney, N.S.W.: Psychology Foundation of Australia; 1995. https://www.worldcat.org/title/manual-for-the-depression-anxiety-stress-scales/oclc/222009504
32.Sahebi A, Asghari MJ, Salari RS. [Validation of Depression Anxiety and Stress Scale (DASS-21) for an Iranian population (Persian)]. J Dev Psychol. 2005; 1(4):36-54. http://jip.azad.ac.ir/article_512443_en.html
33.Haji Amini Z, Zamani M, Fathi Ashtiani A, Ebadi A, Khamseh F, Ghoryehi SH. [Demographic chracteristic correlate to emotional reactions of soldiers (Persian)]. Journal of Military Medicine. 2011; 12(4):211-6. https://www.sid.ir/en/journal/ViewPaper.aspx?id=186925
34.Antony MM, Bieling PJ, Cox Bj, Enns MW, Swinson RP. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety and Stress scales in clinical groups and community sample. Psychological Assessment. 1998; 10:176-81. [DOI:10.1037/1040-3590.10.2.176]
35.Hobart J, Lamping D, Fitzpatrick R, Riazi A, Thompson A. The Multiple Sclerosis Impact Scale (MSIS-29): A new patient-based outcome measure. Brain. 2001; 124(5):962-73. [DOI:10.1093/brain/124.5.962] [PMID]
36.Ramp M, Khan F, Misajon RA, Pallant JF. Rasch analysis of the Multiple Sclerosis Impact Scale (MSIS-29). Health Qual Life Outcomes. 2009; 7:58. [DOI:10.1186/1477-7525-7-58] [PMID] [PMCID]
37.Ayatollahi P, Nafissi Sh, Eshraghian MR, Tarazi A. [Cross-cultural adaptation of the Multiple Sclerosis Impact Scale (MSIS-29) for Iranian MS patients, evaluation of reliability and validity (Persian)]. Tehran Univ Med J. 2006; 64(1):62-8. http://tumj.tums.ac.ir/article-1-1006-en.html
38.Rashid T, Seligman MS. Positive psychotherapy: Clinican manual. Oxfourd: Oxfourd University Press; 2018. https://books.google.com/books?id=09ZjDwAAQBAJ&dq
Received: 2020/08/25 | Accepted: 2020/06/12 | Published: 2020/06/12
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
