Sat, Jan 31, 2026
Volume 11, Issue 4 (Autumn 2025)
Caspian J Neurol Sci 2025, 11(4): 317-328 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khoshsorour S, Narimani M, Basharpour S. Validation of the Persian Version of the Camouflaging Autistic Traits Questionnaire: A Psychometric Evaluation. Caspian J Neurol Sci 2025; 11 (4) :317-328
URL: http://cjns.gums.ac.ir/article-1-750-en.html
URL: http://cjns.gums.ac.ir/article-1-750-en.html



1- Department of Psychology, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
2- Department of Psychology, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran. ,dr.mhdnarimani@gmail.com
2- Department of Psychology, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran. ,
Full-Text [PDF 1711 kb]
(438 Downloads)
| Abstract (HTML) (623 Views)
References
Full-Text: (223 Views)
Introduction
The autism spectrum is characterized by a range of traits, including difficulties in social interaction, stereotyped behaviors, challenges in adapting to change, and heightened attention to detail (AD). These traits reach a clinical threshold in autism spectrum disorder (ASD), but they are also observed in the general population. Consistent with the notion that autistic traits manifest along a continuum, research has shown that relatives of individuals with ASD, as well as some members of the general population, exhibit elevated and subclinical levels of these traits [1]. Autistic traits are present in individuals with typical functioning and may include challenges, such as social interaction difficulties, resistance to change, and sensory sensitivity [2]. Furthermore, individuals with higher levels of autistic traits are more likely to meet the criteria for a clinical diagnosis of ASD [3]. These traits are often studied to understand the increased vulnerability experienced by both autistic and non-autistic individuals, particularly given that many autistic adults remain undiagnosed or misdiagnosed [4].
The prevalence of ASD is notably greater in males compared to females, a difference that is especially pronounced in those with higher intellectual abilities [5]. Recent data from the U.S. Centers for Disease Control and Prevention (CDC) estimate that ASD affects about 1 in 38 eight-year-old boys and 1 in 152 girls of the same age [6]. According to the report, the commonly cited male-to-female ratio of ASD diagnoses is 4:1, yet a relatively larger proportion of males with ASD exhibit average or above-average intellectual functioning compared to females. This discrepancy implies that prevailing conceptions of ASD are disproportionately male-oriented [7]. Women may need to present more numerous or more severe symptoms to obtain a diagnosis, partly because diagnostic measures were initially validated predominantly on male populations [8]. Furthermore, research suggests that females with ASD tend to engage in ‘camouflaging’—a behavior involving the concealment of autistic traits—more frequently than males [9]. This highlights the challenge of identifying ASD symptoms in females, which may lead to misdiagnosis, delayed diagnosis, or no diagnosis, ultimately limiting their access to appropriate treatment and support.
One recent topic that has garnered significant attention in the field of ASD is social camouflaging, which was included in the 11th edition of the international classification of diseases to raise awareness about coping behaviors in the context of autism evaluation [10]. Social camouflaging describes the use of strategies by autistic individuals to downplay their autistic traits in everyday social contexts. This phenomenon is widespread and particularly significant among individuals with higher intellectual abilities [11]. Research has shown that individuals with ASD who do not have intellectual or language impairments tend to have greater awareness of their social challenges. As a result, they often experience symptoms of social anxiety and employ strategies to compensate for these difficulties [12, 13]. Camouflaging autistic traits involves a conscious or unconscious effort to mask or compensate for autistic features, leading to a reduction in overt autistic behaviors [9, 14]. Examples of camouflaging behaviors, as described in the current autism literature, include forcing oneself to maintain eye contact during social interactions, simulating eye contact by directing one’s gaze toward the space between another person’s eyes or the tip of their nose, and employing memory strategies to generate a list of suitable conversation topics. Camouflaging is frequently motivated by the desire to ‘fit in’ and to appear non-autistic [15].
Regarding sex/gender differences, Cage et al. [16] found similar camouflaging autistic traits questionnaire (CAT-Q) scores for men and women with ASD, despite other reports suggesting that women engage in camouflaging more frequently than men, often for practical reasons in work or academic contexts. According to Hull et al. [17], autistic women exhibited higher CAT-Q scores compared to autistic men, whereas no such gender differences were observed among typically developing participants.
Research has shown that social camouflaging has several negative consequences, including reduced access to support and clinical services due to the concealment of related issues. Individuals with higher social camouflaging scores experience increased anxiety and stress, feel distanced from their true selves [9], receive less acceptance from others, and exhibit more symptoms of depression [18]. In a qualitative study involving interviews with late-diagnosed autistic women, feelings of exhaustion and negative impacts on identity were identified as outcomes of social camouflaging [19]. Additionally, social camouflaging has been recognized as a risk factor for suicide in adults with ASD [20].
Apparently, individuals with ASD who do not have intellectual impairments are reported to experience social anxiety more frequently. This increased occurrence may be attributed to a heightened awareness of their social challenges [12, 13, 21]. Additionally, some researchers have linked the use of camouflaging strategies to fewer difficulties in executive functions [22].
In recent years, the timely diagnosis of ASD and the early identification of subthreshold autistic traits have become increasingly important, both therapeutically and in research. A growing number of studies, with diverse objectives, use the CAT-Q to measure social camouflaging, and it appears that the CAT-Q is a promising tool for assessing camouflaging behaviors, which often conceal autistic features in adults and may hinder timely diagnosis, especially among women. In this context, it is essential to make the assessment tool for camouflaging behaviors accessible to non-English speakers and to explore its psychometric properties across different languages and cultures.
Materials and Methods
Study procedure
The present descriptive, cross-sectional study was conducted on male and female students aged 16 to 18 years attending public schools in Tehran during the 2021-2022 academic year. The literature on factor analysis offers several general recommendations concerning appropriate sample sizes, with the majority emphasizing the need for large samples (e.g. at least 200 participants) in order to achieve reliable and valid factor-analytic outcomes [23].
To enhance generalizability, a total of 370 students were selected from the target population using a multistage random sampling method and participated in completing the research instruments. Data collection began with obtaining the necessary permissions. In the first stage of sampling, a complete list of Tehran’s educational districts was compiled, from which Districts 2, 5, and 6 were selected using computer-generated random numbers in Microsoft Excel (RANDBETWEEN function). In the second stage, within each selected district, one boys’ high school and one girls’ high school were randomly chosen using the same method. Finally, in the third stage, two classes were randomly selected from each chosen school to participate in the study. A total of 350 completed questionnaires were included in the final analysis, while 20 were excluded due to incomplete responses.
Eligibility for the current study was determined based on the following criteria: (1) participants must be between 16 and 18 years of age; (2) participants must have no intellectual disability or major cognitive impairment; and (3) participants must provide assent, along with parental or guardian consent.
Participants with a previously identified history of major cognitive impairment or intellectual disability, as reported by parents or school counselors, were excluded from the study. This information was gathered during the initial screening interview to ensure the cognitive eligibility of participants.
The translation process followed the forward-backward method. Initially, the CAT-Q was translated from English into Persian by a team consisting of a PhD in English literature, a psychiatrist, and a psychologist, all of whom were proficient in English. Throughout the translation, expert feedback and linguistic input were systematically incorporated to ensure the accurate preservation of core concepts. Subsequently, the Persian translation underwent back-translation into English by another PhD in English literature. This back-translated version was thoroughly reviewed and revised by the original translation team to ensure conceptual and linguistic accuracy. Finally, the revised Persian version was administered to 10 students to evaluate its grammatical accuracy, fluency, and comprehension difficulty. Based on the feedback and suggestions provided, final revisions were made to ensure the text was fully aligned with the cultural and linguistic context of the target population (Iran) (Appendix A).

Face validity
Face validity was assessed using both quantitative and qualitative approaches. For the qualitative assessment of face validity, 10 specialists in psychology, special education, and psychiatry were selected to review the items and evaluate the statements in terms of comprehensibility, simplicity, and clarity. Their feedback was incorporated, and the items were subsequently revised by the research team to ensure the content remained unchanged. For the quantitative assessment of face validity, the same 10 specialists rated the importance of each item using a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). The importance coefficient for each item was then calculated, and a minimum score of 4.1 was required for the items to be considered valid based on the quantitative assessment.
Content validity
To assess qualitative content validity, expert opinions were solicited. In this study, the instrument was presented to 10 experts in psychology, special education, and psychiatry. They were asked to evaluate the items in terms of grammar, appropriate word usage, item relevance, and proper placement. Based on their feedback, the research team revised certain items while ensuring the core content remained unchanged. For quantitative content validity, expert evaluations were analyzed by calculating two indices: The content validity ratio (CVR) to ensure that the most necessary and relevant items were selected, and the content validity index (CVI) to confirm that the items were appropriately designed to measure the intended content. The minimum acceptable scores for the CVI and CVR were set at 0.7 and 0.6, respectively. As a result, all items were deemed valid.
Study tools
1) CAT-Q: The CAT-Q (Hull et al., 2019) is a self-report instrument consisting of 25 items designed to assess camouflaging strategies [15]. It yields a total score and three subscale scores (also referred to as factors): Compensation (strategies used to compensate for social difficulties related to autism), masking (strategies aimed at concealing autistic traits and/or presenting non-autistic characteristics), and assimilation (strategies intended to adapt to and fit in with non-autistic individuals). Each item is evaluated by respondents on a seven-point Likert scale, with response options spanning from 1 (strongly disagree) to 7 (strongly agree), based on how well each statement describes their social interactions. The total score is calculated by summing the item responses, with appropriate adjustments for reverse-scored items, yielding a possible range from 25 to 175. In the present study, the CAT-Q total and subscale scores were calculated based on the mean of item scores, resulting in scores ranging from 1 to 7. Calculating mean item scores in multi-item Likert scales is a widely accepted approach that enhances the comparability and interpretability of results, especially in statistical analyses, such as factor analysis and regression models [24, 25].
The CAT-Q exhibited satisfactory internal consistency (α=0.94) and showed preliminary evidence of stability over time (r=0.77). Its convergent validity was demonstrated through correlations with well-being, depression, anxiety, and autistic traits [15]. Since the psychometric properties of the CAT-Q have not been examined in Iran, the present study aimed to validate the CAT-Q in the Iranian general population.
2) The social anxiety scale for adolescents (SAS-A): The SAS-A (La Greca & Lopez, 1998) is a self-report instrument developed to evaluate social anxiety in youth populations [26]. The measure consists of 18 core items and 4 filler items, each rated on a five-point Likert scale ranging from 1 (never) to 5 (always). The scale yields three subscales: Fear of negative evaluation (FNE; 8 items), social avoidance and distress in novel situations (SAD-new; 6 items), and generalized social avoidance and distress (SAD-general; 4 items). Subscale and total scale scores are derived by summing adolescents’ ratings for each item. The score ranges for the subscales are as follows: 8–40 for FNE, 6–30 for SAD-new, and 4–20 for SAD-general, while the overall SAS-A score ranges from 18 to 90. Higher scores indicate greater severity of social anxiety. Research has shown satisfactory internal consistency, with Cronbach’s α values ranging from 0.76 to 0.91. Test re-test reliability over a two-month period has been reported within the range of 0.54 to 0.78 [26, 27]. The SAS-A also demonstrates good construct validity, supported by significant correlations with other instruments assessing general or unspecified anxiety and depressive symptoms [28]. In Iran, Ostvar and Razavieh [29] reported a test re-test reliability of 0.88 for the overall scale, and Cronbach’s α values for the subscales FNE, SAD-New, and SAD-general as 0.84, 0.74, and 0.77, respectively.
3) Autism-spectrum quotient (AQ): The AQ (Baron-Cohen et al., 2001) is a 50-item self-report measure developed to evaluate autistic traits in both clinical populations and the general community. Items are rated on a four-point Likert scale, and the AQ yields five subscales: AD, attention switching (AS), social skills (SS), communication (C), and imagination (I). Responses indicating more autistic traits are scored as 1, while responses indicating non-autistic traits are scored as 0. The AQ yields a total score ranging from 0 to 50, where higher values indicate greater severity of autistic traits. Psychometric evaluations of the instrument have demonstrated strong test re-test reliability and acceptable-to-high internal consistency [30]. In Iran, Nejati Safa et al. [31] reported a Cronbach’s α of 0.79 for the total score, indicating acceptable internal consistency.
Statistical analysis
Participants were initially categorized into three groups based on their autistic traits, as measured by the AQ. Group 1, termed the ‘low-AT group,’ included individuals who scored below 19 on the AQ (n=151). Group 2, referred to as the ‘mid-AT group,’ comprised participants with scores ranging from 19 to 31 (n=147). Group 3, called the ‘high-AT group,’ consisted of individuals who scored 32 or higher (n=52). The threshold score of 32 for the ‘high’ scoring group was based on the original study by Baron-Cohen et al. [30], where this score marked the point at which 80% of individuals with autism scored. Additionally, following Robertson & Simmons [32], the minimum score for the ‘Mid’ group was set at 19 to ensure the inclusion of individuals with higher-than-average AQ scores, considering the mean AQ score of 16.4 for controls in the original AQ study [30].
Cronbach’s α was used to estimate the internal consistency of the CAT-Q (n=40). Construct validity was examined by applying Pearson’s correlations, both across the three subscales and between individual subscales and the overall CAT-Q score. Test re-test reliability of the CAT-Q was determined using the intraclass correlation coefficient (ICC). To assess test re-test reliability, 25 participants from the original sample were asked to complete the questionnaire once again after a two-month interval. Given that the questionnaire was self-administered in both sessions, no external raters were involved in the evaluation process. Consequently, a two-way mixed-effects model with absolute agreement for single measurements was utilized to compute the ICC. The resulting value (ICC=0.821) indicated a high degree of test re-test reliability, reflecting the stability and consistency of the measurement over time.
To assess the representativeness of the re-test group compared to the total sample, the distributions of gender, grade, and age were compared between the two groups. The chi-square test indicated no significant differences between the re-test group (n=25) and the total sample (n=350) in terms of gender (χ²(1)=0.027, P=0.87), grade (χ²(2)=0.108, P=0.95), and age (χ²(2)=0.138, P=0.93). Therefore, it can be concluded that the re-test group was a good representation of the total study population.
To evaluate convergent validity, Pearson’s correlation coefficients were used, relating CAT-Q total and subscale scores to those obtained from the AQ and SAS-A. The SAS-A was included to assess convergent validity based on prior evidence indicating that a significant proportion (29–57%) of autistic youth experience co-occurring social anxiety disorder (SAD) [33]. Social camouflaging and the safety behaviors associated with social anxiety both involve efforts to conceal one’s authentic self to avoid negative social evaluation, suggesting conceptual overlap between these constructs.
Subsequently, known-groups validity was assessed by comparing CAT-Q scores—both total and individual factor scores—across the three groups: low-AT, mid-AT, and high-AT, using one-way ANOVA. Bonferroni-corrected post hoc comparisons were also conducted. Statistical analyses were carried out using SPSS software, version 23.
Results
The study sample comprised 350 high school students, of whom 230 were female and 120 were male. The Mean±SD age of participants was 17.05±0.71 years. Sex distribution did not vary significantly across the groups. A significant difference was found in the mean AQ scores among the three groups, with the low-AT group exhibiting significantly lower mean scores compared to the other two groups. Additionally, a significant difference emerged in SAS-A averages between the high-AT and low-AT groups, with the high-AT group reporting elevated levels of social anxiety (Table 1).

Effect size estimates indicated a very large effect for AQ (η²=0.85), a small effect for SAS-A (η²=0.02), and a negligible association for sex distribution (Cramér’s V=0.04).
Reliability
Internal consistency for the CAT-Q was high (Cronbach’s α=0.883). Each of its subscales (compensation, masking, and assimilation) yielded α values greater than 0.70 (Table 2).

The three subscales exhibited substantial correlations with the total score, and significant positive correlations were found among the subscales themselves (Table 3).

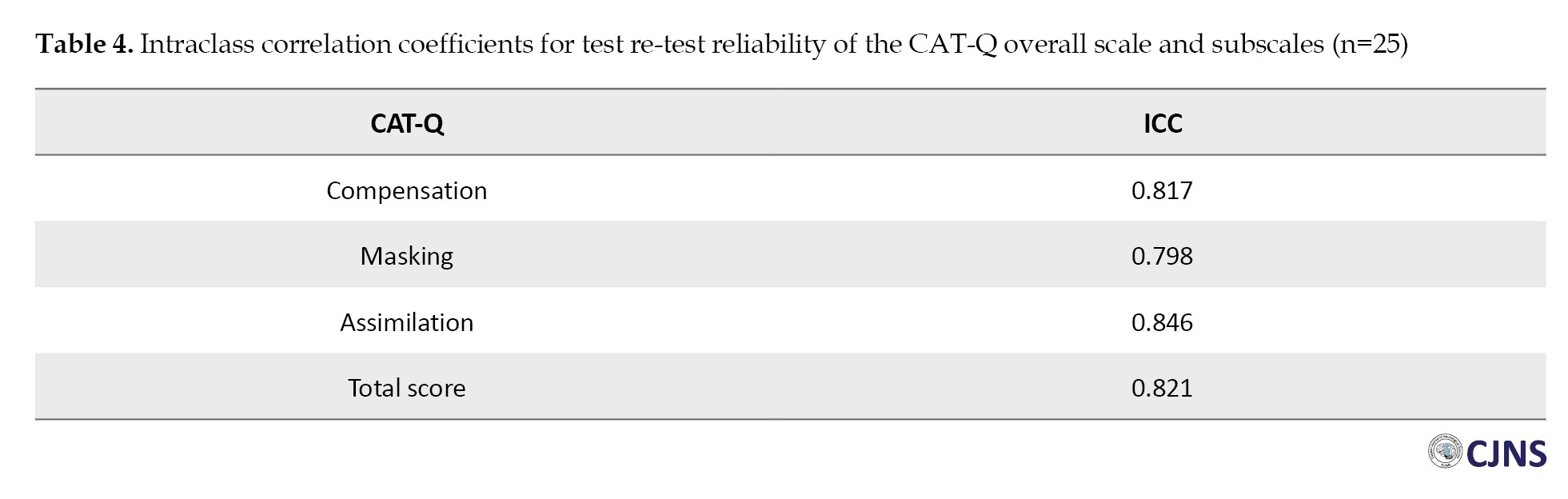
The ICCs obtained for each CAT-Q subscale, as well as for the total score, were above 0.75, supporting the measure’s test re-test reliability (Table 4).
Convergent validity
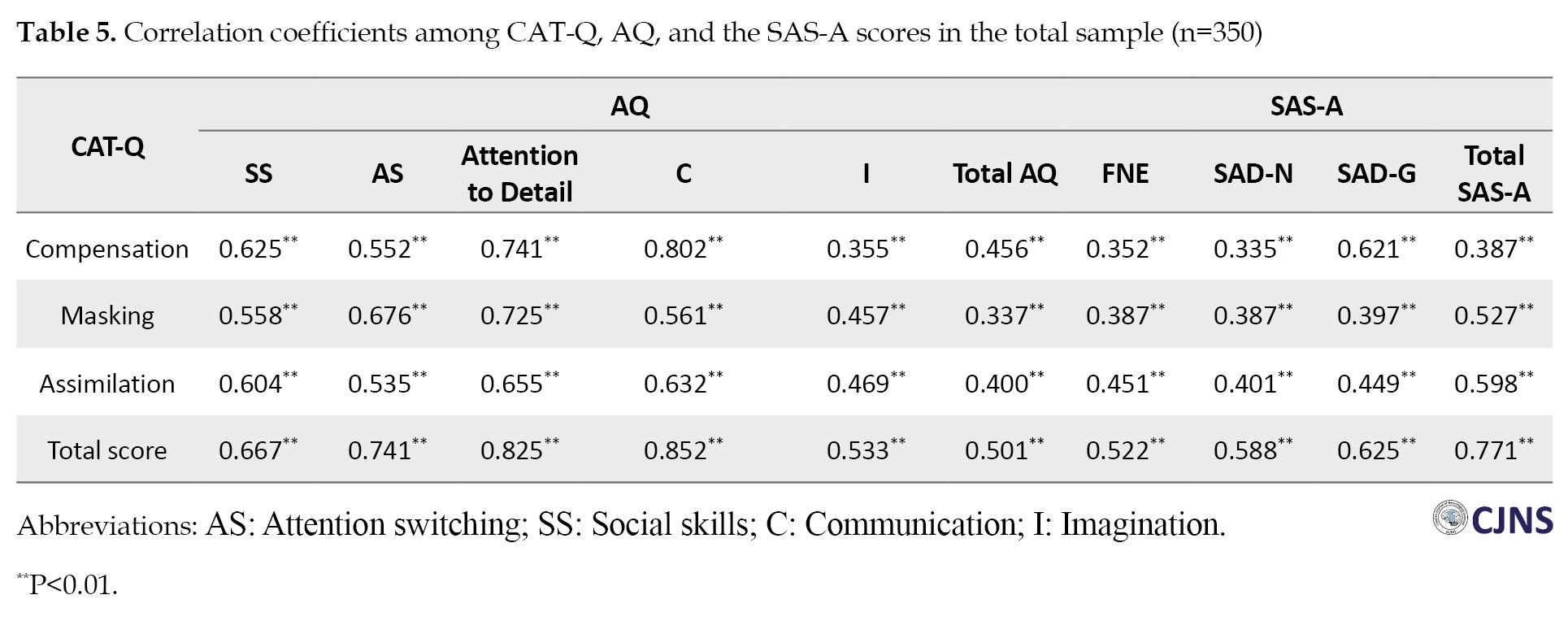
The total score of the CAT-Q was significantly associated with the total score of the AQ (r=0.501). Each of the three CAT-Q factors demonstrated significant correlations with the AQ total score. The weakest correlation was observed for the CAT-Q masking factor (r=0.337), while the strongest correlation was found with the CAT-Q compensation factor (r=0.456). Additionally, the CAT-Q total score was significantly correlated with all AQ subscale scores, with correlations ranging from moderate for the I subscale (r=0.533) to strong for the C subscale (r=0.852). All relationships between the CAT-Q factors and AQ subscales were positive and statistically significant.
The CAT-Q total score also exhibited a significant and strong correlation with the SAS-A total score (r=0.771). Each of the CAT-Q factors showed positive and significant correlations with the SAS-A total score. The weakest correlation was observed with the CAT-Q compensation factor (r=0.387), while the strongest was found with the CAT-Q assimilation factor (r=0.598). Furthermore, the CAT-Q total score displayed significant correlations with all SAS-A subscale scores, ranging from moderate for the FNE subscale (r=0.522) to strong for the SAD-G subscale (r=0.625) (Table 5).
Known-groups validity
Participants were categorized based on their autistic trait levels as measured by the AQ. ANOVA results indicated significant group differences in the CAT-Q total score as well as across all subscales. Bonferroni-adjusted post-hoc analyses showed that the high-AT group obtained markedly higher scores than both the mid-AT and low-AT groups. Moreover, the mid-AT group also demonstrated higher mean scores relative to the low-AT group (Table 6).

Effect size estimates indicated large effects for the CAT-Q total score (η²=0.26) and compensation (η²=0.22), a moderate-to-large effect for assimilation (η²=0.16), and a moderate effect for masking (η²=0.06).
Discussion
In the present research, we sought to examine the psychometric properties of the Persian adaptation of the CAT-Q within a student sample. Previous studies by Hull et al. [9, 15] emphasized that the CAT-Q is an effective measure for capturing camouflaging strategies—behaviors that can mask autistic characteristics and complicate the diagnosis of ASD, especially in females. The recent emphasis by clinicians and researchers on the importance of timely ASD diagnosis and the early recognition of subthreshold autistic traits highlights the need to extend camouflaging measures to non-English-speaking populations [9, 15].
In the present study, the instrument demonstrated satisfactory internal consistency at both the whole scale and subscale levels. Specifically, the lowest value, which is consistent with the original validation study, was observed for the masking factor. Additionally, strong correlations were identified between the CAT-Q total scores and the scores of individual factors. The test re-test reliability was acceptable, affirming the instrument’s reliability within our sample.
In line with expectations, participants in the high-AT group—those presenting with clinical manifestations of ASD—exhibited elevated levels of camouflaging behaviors on the CAT-Q. Participants in the mid-AT group—those with subthreshold traits—reported moderate levels, while participants in the low-AT group—those with low autistic traits—exhibited the lowest camouflaging scores. These findings may be regarded as supporting the interpretation that camouflaging occurs on a continuum from the general population to clinical samples, consistent with the continuous nature of the autism spectrum [13, 15].
The total CAT-Q score showed a positive correlation with autistic-like traits, suggesting that individuals exhibiting elevated levels of these traits tend to display camouflaging behaviors, regardless of an autism diagnosis. Given that proficient camouflaging at high levels may lead to missed clinical diagnoses [34], utilizing the CAT-Q could be valuable in identifying camouflaging behaviors among people considered at risk for autism, even if they have not yet met the formal diagnostic criteria.
Our findings revealed significant correlations between all CAT-Q subscales and the subscales of the AQ and the SAS-A, consistent with the results reported by Hull et al. [15]. They observed higher correlations of the CAT-Q with the broad autism phenotype questionnaire (BAP-Q) and the Liebowitz social anxiety scale (LSAS) [9, 15].
Within the cognitive model proposed by Clark and Wells [33], individuals with SAD engage in safety behaviors—strategic efforts to minimize perceived social-evaluative threats. These behaviors are classified as avoidance (e.g. avoiding eye contact) and impression management (e.g. appearing more sociable). While both can maintain anxiety, avoidance tends to impair social interactions more severely, as it is often perceived more negatively by others. The use of safety behaviors to conceal one’s social anxiety parallels the concept of social camouflaging in autism [35]. Camouflaging encompasses a range of compensation strategies aimed at addressing social and C challenges in autism, masking techniques that facilitate the presentation of a non-autistic persona to neurotypical peers, and assimilation strategies designed to help individuals navigate potentially uncomfortable social situations [33]. This conceptual overlap between social camouflaging and social anxiety supports the use of the SAS-A to evaluate the convergent validity of the CAT-Q. Both constructs reflect efforts to conceal one’s authentic self in social contexts, highlighting the utility of the SAS-A as a convergent measure in validating the CAT-Q.
In addition to the validation of the Persian version, the CAT-Q has been tested across various cultural contexts, showing promising results in different populations. The CAT-Q has been evaluated with university students in Italy and with autistic and non-autistic adults in the UK, demonstrating good validity and internal consistency [36, 15]. However, the French and Dutch versions exhibited reliable but inconsistent measurements across autistic and non-autistic adults [37, 38]. The Japanese version demonstrated sufficient internal consistency for both autistic and non-autistic samples, along with moderate-to-good and consistent test re-test reliability across all three subscales [39]. The Taiwanese version, examined among autistic and non-autistic children, adolescents, and their caregivers, demonstrated a two-factor structure—compensation/masking and assimilation—with satisfactory reliability [40]. In the Persian version, the CAT-Q demonstrated a good fit to the primary three-factor structure. Furthermore, it exhibited acceptable internal consistency, satisfactory test re-test reliability, and strong evidence of content validity, known-groups validity, and convergent validity.
It is important to interpret the results of this study within the context of certain limitations. Specifically, our sample consisted primarily of school students, which may limit the generalizability of the findings to the broader population. To strengthen the external validity of our conclusions regarding the CAT-Q’s effectiveness in assessing camouflaging behaviors, further research involving more diverse, general population samples—ideally with clinical assessments—is needed. Furthermore, validating the instrument in clinical settings, particularly with individuals who have a confirmed autism diagnosis, is essential for ensuring its applicability in these contexts.
It is also important to consider that the self-report nature of the CAT-Q relies on individuals’ self-reflection and their ability to articulate their camouflaging behaviors and motivations. As a result, its applicability may be limited for those who have difficulty reflecting on their behaviors or expressing their motivations, such as some autistic individuals with language or intellectual challenges. To address this limitation, the CAT-Q can be supplemented with behavioral observations or informant-report measures of camouflaging. This combined approach allows for the assessment of camouflaging behaviors in individuals with limited self-insight or C abilities. By integrating the CAT-Q with observed behavioral and cognitive measures, a more comprehensive evaluation of this complex phenomenon can be achieved.
In the present study, given that group classification was based on AQ cut-offs, the high-AT group was comparatively smaller (n=52). This distribution is expected in community-based samples. Nonetheless, the total sample size (n=350) was sufficient for the psychometric analyses conducted.
Conclusion
The CAT-Q demonstrates its reliability and validity as an effective instrument for assessing social camouflaging behaviors. It shows considerable potential as a valuable tool for future research within Iranian populations, contributing to a better understanding of how social camouflaging manifests in this context. The CAT-Q’s ability to provide both theoretical and practical insights makes it a crucial tool for advancing research on social camouflaging, highlighting its importance for future studies in this field.
Ethical Considerations
Compliance with ethical guidelines
All research procedures were conducted in accordance with the ethical standards outlined in the 2013 Declaration of Helsinki. This study was approved by the Research Ethics Committee of the University of Mohaghegh Ardabili, Ardabil, Iran (Code: IR.UMA.REC.1403.052). Participation was fully voluntary, with written consent obtained from parents or legal guardians, alongside assent from the adolescent participants prior to data collection.
Funding
This study was extracted from the PhD dissertation of Sahar Khoshsorour, approved by the Department of Psychology, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran. This research did not receive any specific funding from public, commercial, or non-profit sector funding agencies.
Authors contributions
Data collection, statistical analyses, and writing the original draft: Sahar Khoshsorour; Review and editing: Mohammad Narimani and Sajjad Beshrpour; Conceptualization, methodology, and final approval: All authors; Supervision: Mohammad Narimani.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors gratefully acknowledge all the participants who generously dedicated their time and effort to complete the questionnaires for this study. Their valuable contributions have been instrumental in advancing our understanding of this field. The authors also extend their appreciation to the Education Departments of Districts 2, 5, and 6 of Tehran, who facilitated the recruitment of participants and supported the data collection process.
The autism spectrum is characterized by a range of traits, including difficulties in social interaction, stereotyped behaviors, challenges in adapting to change, and heightened attention to detail (AD). These traits reach a clinical threshold in autism spectrum disorder (ASD), but they are also observed in the general population. Consistent with the notion that autistic traits manifest along a continuum, research has shown that relatives of individuals with ASD, as well as some members of the general population, exhibit elevated and subclinical levels of these traits [1]. Autistic traits are present in individuals with typical functioning and may include challenges, such as social interaction difficulties, resistance to change, and sensory sensitivity [2]. Furthermore, individuals with higher levels of autistic traits are more likely to meet the criteria for a clinical diagnosis of ASD [3]. These traits are often studied to understand the increased vulnerability experienced by both autistic and non-autistic individuals, particularly given that many autistic adults remain undiagnosed or misdiagnosed [4].
The prevalence of ASD is notably greater in males compared to females, a difference that is especially pronounced in those with higher intellectual abilities [5]. Recent data from the U.S. Centers for Disease Control and Prevention (CDC) estimate that ASD affects about 1 in 38 eight-year-old boys and 1 in 152 girls of the same age [6]. According to the report, the commonly cited male-to-female ratio of ASD diagnoses is 4:1, yet a relatively larger proportion of males with ASD exhibit average or above-average intellectual functioning compared to females. This discrepancy implies that prevailing conceptions of ASD are disproportionately male-oriented [7]. Women may need to present more numerous or more severe symptoms to obtain a diagnosis, partly because diagnostic measures were initially validated predominantly on male populations [8]. Furthermore, research suggests that females with ASD tend to engage in ‘camouflaging’—a behavior involving the concealment of autistic traits—more frequently than males [9]. This highlights the challenge of identifying ASD symptoms in females, which may lead to misdiagnosis, delayed diagnosis, or no diagnosis, ultimately limiting their access to appropriate treatment and support.
One recent topic that has garnered significant attention in the field of ASD is social camouflaging, which was included in the 11th edition of the international classification of diseases to raise awareness about coping behaviors in the context of autism evaluation [10]. Social camouflaging describes the use of strategies by autistic individuals to downplay their autistic traits in everyday social contexts. This phenomenon is widespread and particularly significant among individuals with higher intellectual abilities [11]. Research has shown that individuals with ASD who do not have intellectual or language impairments tend to have greater awareness of their social challenges. As a result, they often experience symptoms of social anxiety and employ strategies to compensate for these difficulties [12, 13]. Camouflaging autistic traits involves a conscious or unconscious effort to mask or compensate for autistic features, leading to a reduction in overt autistic behaviors [9, 14]. Examples of camouflaging behaviors, as described in the current autism literature, include forcing oneself to maintain eye contact during social interactions, simulating eye contact by directing one’s gaze toward the space between another person’s eyes or the tip of their nose, and employing memory strategies to generate a list of suitable conversation topics. Camouflaging is frequently motivated by the desire to ‘fit in’ and to appear non-autistic [15].
Regarding sex/gender differences, Cage et al. [16] found similar camouflaging autistic traits questionnaire (CAT-Q) scores for men and women with ASD, despite other reports suggesting that women engage in camouflaging more frequently than men, often for practical reasons in work or academic contexts. According to Hull et al. [17], autistic women exhibited higher CAT-Q scores compared to autistic men, whereas no such gender differences were observed among typically developing participants.
Research has shown that social camouflaging has several negative consequences, including reduced access to support and clinical services due to the concealment of related issues. Individuals with higher social camouflaging scores experience increased anxiety and stress, feel distanced from their true selves [9], receive less acceptance from others, and exhibit more symptoms of depression [18]. In a qualitative study involving interviews with late-diagnosed autistic women, feelings of exhaustion and negative impacts on identity were identified as outcomes of social camouflaging [19]. Additionally, social camouflaging has been recognized as a risk factor for suicide in adults with ASD [20].
Apparently, individuals with ASD who do not have intellectual impairments are reported to experience social anxiety more frequently. This increased occurrence may be attributed to a heightened awareness of their social challenges [12, 13, 21]. Additionally, some researchers have linked the use of camouflaging strategies to fewer difficulties in executive functions [22].
In recent years, the timely diagnosis of ASD and the early identification of subthreshold autistic traits have become increasingly important, both therapeutically and in research. A growing number of studies, with diverse objectives, use the CAT-Q to measure social camouflaging, and it appears that the CAT-Q is a promising tool for assessing camouflaging behaviors, which often conceal autistic features in adults and may hinder timely diagnosis, especially among women. In this context, it is essential to make the assessment tool for camouflaging behaviors accessible to non-English speakers and to explore its psychometric properties across different languages and cultures.
Materials and Methods
Study procedure
The present descriptive, cross-sectional study was conducted on male and female students aged 16 to 18 years attending public schools in Tehran during the 2021-2022 academic year. The literature on factor analysis offers several general recommendations concerning appropriate sample sizes, with the majority emphasizing the need for large samples (e.g. at least 200 participants) in order to achieve reliable and valid factor-analytic outcomes [23].
To enhance generalizability, a total of 370 students were selected from the target population using a multistage random sampling method and participated in completing the research instruments. Data collection began with obtaining the necessary permissions. In the first stage of sampling, a complete list of Tehran’s educational districts was compiled, from which Districts 2, 5, and 6 were selected using computer-generated random numbers in Microsoft Excel (RANDBETWEEN function). In the second stage, within each selected district, one boys’ high school and one girls’ high school were randomly chosen using the same method. Finally, in the third stage, two classes were randomly selected from each chosen school to participate in the study. A total of 350 completed questionnaires were included in the final analysis, while 20 were excluded due to incomplete responses.
Eligibility for the current study was determined based on the following criteria: (1) participants must be between 16 and 18 years of age; (2) participants must have no intellectual disability or major cognitive impairment; and (3) participants must provide assent, along with parental or guardian consent.
Participants with a previously identified history of major cognitive impairment or intellectual disability, as reported by parents or school counselors, were excluded from the study. This information was gathered during the initial screening interview to ensure the cognitive eligibility of participants.
The translation process followed the forward-backward method. Initially, the CAT-Q was translated from English into Persian by a team consisting of a PhD in English literature, a psychiatrist, and a psychologist, all of whom were proficient in English. Throughout the translation, expert feedback and linguistic input were systematically incorporated to ensure the accurate preservation of core concepts. Subsequently, the Persian translation underwent back-translation into English by another PhD in English literature. This back-translated version was thoroughly reviewed and revised by the original translation team to ensure conceptual and linguistic accuracy. Finally, the revised Persian version was administered to 10 students to evaluate its grammatical accuracy, fluency, and comprehension difficulty. Based on the feedback and suggestions provided, final revisions were made to ensure the text was fully aligned with the cultural and linguistic context of the target population (Iran) (Appendix A).
Face validity
Face validity was assessed using both quantitative and qualitative approaches. For the qualitative assessment of face validity, 10 specialists in psychology, special education, and psychiatry were selected to review the items and evaluate the statements in terms of comprehensibility, simplicity, and clarity. Their feedback was incorporated, and the items were subsequently revised by the research team to ensure the content remained unchanged. For the quantitative assessment of face validity, the same 10 specialists rated the importance of each item using a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). The importance coefficient for each item was then calculated, and a minimum score of 4.1 was required for the items to be considered valid based on the quantitative assessment.
Content validity
To assess qualitative content validity, expert opinions were solicited. In this study, the instrument was presented to 10 experts in psychology, special education, and psychiatry. They were asked to evaluate the items in terms of grammar, appropriate word usage, item relevance, and proper placement. Based on their feedback, the research team revised certain items while ensuring the core content remained unchanged. For quantitative content validity, expert evaluations were analyzed by calculating two indices: The content validity ratio (CVR) to ensure that the most necessary and relevant items were selected, and the content validity index (CVI) to confirm that the items were appropriately designed to measure the intended content. The minimum acceptable scores for the CVI and CVR were set at 0.7 and 0.6, respectively. As a result, all items were deemed valid.
Study tools
1) CAT-Q: The CAT-Q (Hull et al., 2019) is a self-report instrument consisting of 25 items designed to assess camouflaging strategies [15]. It yields a total score and three subscale scores (also referred to as factors): Compensation (strategies used to compensate for social difficulties related to autism), masking (strategies aimed at concealing autistic traits and/or presenting non-autistic characteristics), and assimilation (strategies intended to adapt to and fit in with non-autistic individuals). Each item is evaluated by respondents on a seven-point Likert scale, with response options spanning from 1 (strongly disagree) to 7 (strongly agree), based on how well each statement describes their social interactions. The total score is calculated by summing the item responses, with appropriate adjustments for reverse-scored items, yielding a possible range from 25 to 175. In the present study, the CAT-Q total and subscale scores were calculated based on the mean of item scores, resulting in scores ranging from 1 to 7. Calculating mean item scores in multi-item Likert scales is a widely accepted approach that enhances the comparability and interpretability of results, especially in statistical analyses, such as factor analysis and regression models [24, 25].
The CAT-Q exhibited satisfactory internal consistency (α=0.94) and showed preliminary evidence of stability over time (r=0.77). Its convergent validity was demonstrated through correlations with well-being, depression, anxiety, and autistic traits [15]. Since the psychometric properties of the CAT-Q have not been examined in Iran, the present study aimed to validate the CAT-Q in the Iranian general population.
2) The social anxiety scale for adolescents (SAS-A): The SAS-A (La Greca & Lopez, 1998) is a self-report instrument developed to evaluate social anxiety in youth populations [26]. The measure consists of 18 core items and 4 filler items, each rated on a five-point Likert scale ranging from 1 (never) to 5 (always). The scale yields three subscales: Fear of negative evaluation (FNE; 8 items), social avoidance and distress in novel situations (SAD-new; 6 items), and generalized social avoidance and distress (SAD-general; 4 items). Subscale and total scale scores are derived by summing adolescents’ ratings for each item. The score ranges for the subscales are as follows: 8–40 for FNE, 6–30 for SAD-new, and 4–20 for SAD-general, while the overall SAS-A score ranges from 18 to 90. Higher scores indicate greater severity of social anxiety. Research has shown satisfactory internal consistency, with Cronbach’s α values ranging from 0.76 to 0.91. Test re-test reliability over a two-month period has been reported within the range of 0.54 to 0.78 [26, 27]. The SAS-A also demonstrates good construct validity, supported by significant correlations with other instruments assessing general or unspecified anxiety and depressive symptoms [28]. In Iran, Ostvar and Razavieh [29] reported a test re-test reliability of 0.88 for the overall scale, and Cronbach’s α values for the subscales FNE, SAD-New, and SAD-general as 0.84, 0.74, and 0.77, respectively.
3) Autism-spectrum quotient (AQ): The AQ (Baron-Cohen et al., 2001) is a 50-item self-report measure developed to evaluate autistic traits in both clinical populations and the general community. Items are rated on a four-point Likert scale, and the AQ yields five subscales: AD, attention switching (AS), social skills (SS), communication (C), and imagination (I). Responses indicating more autistic traits are scored as 1, while responses indicating non-autistic traits are scored as 0. The AQ yields a total score ranging from 0 to 50, where higher values indicate greater severity of autistic traits. Psychometric evaluations of the instrument have demonstrated strong test re-test reliability and acceptable-to-high internal consistency [30]. In Iran, Nejati Safa et al. [31] reported a Cronbach’s α of 0.79 for the total score, indicating acceptable internal consistency.
Statistical analysis
Participants were initially categorized into three groups based on their autistic traits, as measured by the AQ. Group 1, termed the ‘low-AT group,’ included individuals who scored below 19 on the AQ (n=151). Group 2, referred to as the ‘mid-AT group,’ comprised participants with scores ranging from 19 to 31 (n=147). Group 3, called the ‘high-AT group,’ consisted of individuals who scored 32 or higher (n=52). The threshold score of 32 for the ‘high’ scoring group was based on the original study by Baron-Cohen et al. [30], where this score marked the point at which 80% of individuals with autism scored. Additionally, following Robertson & Simmons [32], the minimum score for the ‘Mid’ group was set at 19 to ensure the inclusion of individuals with higher-than-average AQ scores, considering the mean AQ score of 16.4 for controls in the original AQ study [30].
Cronbach’s α was used to estimate the internal consistency of the CAT-Q (n=40). Construct validity was examined by applying Pearson’s correlations, both across the three subscales and between individual subscales and the overall CAT-Q score. Test re-test reliability of the CAT-Q was determined using the intraclass correlation coefficient (ICC). To assess test re-test reliability, 25 participants from the original sample were asked to complete the questionnaire once again after a two-month interval. Given that the questionnaire was self-administered in both sessions, no external raters were involved in the evaluation process. Consequently, a two-way mixed-effects model with absolute agreement for single measurements was utilized to compute the ICC. The resulting value (ICC=0.821) indicated a high degree of test re-test reliability, reflecting the stability and consistency of the measurement over time.
To assess the representativeness of the re-test group compared to the total sample, the distributions of gender, grade, and age were compared between the two groups. The chi-square test indicated no significant differences between the re-test group (n=25) and the total sample (n=350) in terms of gender (χ²(1)=0.027, P=0.87), grade (χ²(2)=0.108, P=0.95), and age (χ²(2)=0.138, P=0.93). Therefore, it can be concluded that the re-test group was a good representation of the total study population.
To evaluate convergent validity, Pearson’s correlation coefficients were used, relating CAT-Q total and subscale scores to those obtained from the AQ and SAS-A. The SAS-A was included to assess convergent validity based on prior evidence indicating that a significant proportion (29–57%) of autistic youth experience co-occurring social anxiety disorder (SAD) [33]. Social camouflaging and the safety behaviors associated with social anxiety both involve efforts to conceal one’s authentic self to avoid negative social evaluation, suggesting conceptual overlap between these constructs.
Subsequently, known-groups validity was assessed by comparing CAT-Q scores—both total and individual factor scores—across the three groups: low-AT, mid-AT, and high-AT, using one-way ANOVA. Bonferroni-corrected post hoc comparisons were also conducted. Statistical analyses were carried out using SPSS software, version 23.
Results
The study sample comprised 350 high school students, of whom 230 were female and 120 were male. The Mean±SD age of participants was 17.05±0.71 years. Sex distribution did not vary significantly across the groups. A significant difference was found in the mean AQ scores among the three groups, with the low-AT group exhibiting significantly lower mean scores compared to the other two groups. Additionally, a significant difference emerged in SAS-A averages between the high-AT and low-AT groups, with the high-AT group reporting elevated levels of social anxiety (Table 1).
Effect size estimates indicated a very large effect for AQ (η²=0.85), a small effect for SAS-A (η²=0.02), and a negligible association for sex distribution (Cramér’s V=0.04).
Reliability
Internal consistency for the CAT-Q was high (Cronbach’s α=0.883). Each of its subscales (compensation, masking, and assimilation) yielded α values greater than 0.70 (Table 2).
The three subscales exhibited substantial correlations with the total score, and significant positive correlations were found among the subscales themselves (Table 3).
The ICCs obtained for each CAT-Q subscale, as well as for the total score, were above 0.75, supporting the measure’s test re-test reliability (Table 4).
Convergent validity
The total score of the CAT-Q was significantly associated with the total score of the AQ (r=0.501). Each of the three CAT-Q factors demonstrated significant correlations with the AQ total score. The weakest correlation was observed for the CAT-Q masking factor (r=0.337), while the strongest correlation was found with the CAT-Q compensation factor (r=0.456). Additionally, the CAT-Q total score was significantly correlated with all AQ subscale scores, with correlations ranging from moderate for the I subscale (r=0.533) to strong for the C subscale (r=0.852). All relationships between the CAT-Q factors and AQ subscales were positive and statistically significant.
The CAT-Q total score also exhibited a significant and strong correlation with the SAS-A total score (r=0.771). Each of the CAT-Q factors showed positive and significant correlations with the SAS-A total score. The weakest correlation was observed with the CAT-Q compensation factor (r=0.387), while the strongest was found with the CAT-Q assimilation factor (r=0.598). Furthermore, the CAT-Q total score displayed significant correlations with all SAS-A subscale scores, ranging from moderate for the FNE subscale (r=0.522) to strong for the SAD-G subscale (r=0.625) (Table 5).
Known-groups validity
Participants were categorized based on their autistic trait levels as measured by the AQ. ANOVA results indicated significant group differences in the CAT-Q total score as well as across all subscales. Bonferroni-adjusted post-hoc analyses showed that the high-AT group obtained markedly higher scores than both the mid-AT and low-AT groups. Moreover, the mid-AT group also demonstrated higher mean scores relative to the low-AT group (Table 6).
Effect size estimates indicated large effects for the CAT-Q total score (η²=0.26) and compensation (η²=0.22), a moderate-to-large effect for assimilation (η²=0.16), and a moderate effect for masking (η²=0.06).
Discussion
In the present research, we sought to examine the psychometric properties of the Persian adaptation of the CAT-Q within a student sample. Previous studies by Hull et al. [9, 15] emphasized that the CAT-Q is an effective measure for capturing camouflaging strategies—behaviors that can mask autistic characteristics and complicate the diagnosis of ASD, especially in females. The recent emphasis by clinicians and researchers on the importance of timely ASD diagnosis and the early recognition of subthreshold autistic traits highlights the need to extend camouflaging measures to non-English-speaking populations [9, 15].
In the present study, the instrument demonstrated satisfactory internal consistency at both the whole scale and subscale levels. Specifically, the lowest value, which is consistent with the original validation study, was observed for the masking factor. Additionally, strong correlations were identified between the CAT-Q total scores and the scores of individual factors. The test re-test reliability was acceptable, affirming the instrument’s reliability within our sample.
In line with expectations, participants in the high-AT group—those presenting with clinical manifestations of ASD—exhibited elevated levels of camouflaging behaviors on the CAT-Q. Participants in the mid-AT group—those with subthreshold traits—reported moderate levels, while participants in the low-AT group—those with low autistic traits—exhibited the lowest camouflaging scores. These findings may be regarded as supporting the interpretation that camouflaging occurs on a continuum from the general population to clinical samples, consistent with the continuous nature of the autism spectrum [13, 15].
The total CAT-Q score showed a positive correlation with autistic-like traits, suggesting that individuals exhibiting elevated levels of these traits tend to display camouflaging behaviors, regardless of an autism diagnosis. Given that proficient camouflaging at high levels may lead to missed clinical diagnoses [34], utilizing the CAT-Q could be valuable in identifying camouflaging behaviors among people considered at risk for autism, even if they have not yet met the formal diagnostic criteria.
Our findings revealed significant correlations between all CAT-Q subscales and the subscales of the AQ and the SAS-A, consistent with the results reported by Hull et al. [15]. They observed higher correlations of the CAT-Q with the broad autism phenotype questionnaire (BAP-Q) and the Liebowitz social anxiety scale (LSAS) [9, 15].
Within the cognitive model proposed by Clark and Wells [33], individuals with SAD engage in safety behaviors—strategic efforts to minimize perceived social-evaluative threats. These behaviors are classified as avoidance (e.g. avoiding eye contact) and impression management (e.g. appearing more sociable). While both can maintain anxiety, avoidance tends to impair social interactions more severely, as it is often perceived more negatively by others. The use of safety behaviors to conceal one’s social anxiety parallels the concept of social camouflaging in autism [35]. Camouflaging encompasses a range of compensation strategies aimed at addressing social and C challenges in autism, masking techniques that facilitate the presentation of a non-autistic persona to neurotypical peers, and assimilation strategies designed to help individuals navigate potentially uncomfortable social situations [33]. This conceptual overlap between social camouflaging and social anxiety supports the use of the SAS-A to evaluate the convergent validity of the CAT-Q. Both constructs reflect efforts to conceal one’s authentic self in social contexts, highlighting the utility of the SAS-A as a convergent measure in validating the CAT-Q.
In addition to the validation of the Persian version, the CAT-Q has been tested across various cultural contexts, showing promising results in different populations. The CAT-Q has been evaluated with university students in Italy and with autistic and non-autistic adults in the UK, demonstrating good validity and internal consistency [36, 15]. However, the French and Dutch versions exhibited reliable but inconsistent measurements across autistic and non-autistic adults [37, 38]. The Japanese version demonstrated sufficient internal consistency for both autistic and non-autistic samples, along with moderate-to-good and consistent test re-test reliability across all three subscales [39]. The Taiwanese version, examined among autistic and non-autistic children, adolescents, and their caregivers, demonstrated a two-factor structure—compensation/masking and assimilation—with satisfactory reliability [40]. In the Persian version, the CAT-Q demonstrated a good fit to the primary three-factor structure. Furthermore, it exhibited acceptable internal consistency, satisfactory test re-test reliability, and strong evidence of content validity, known-groups validity, and convergent validity.
It is important to interpret the results of this study within the context of certain limitations. Specifically, our sample consisted primarily of school students, which may limit the generalizability of the findings to the broader population. To strengthen the external validity of our conclusions regarding the CAT-Q’s effectiveness in assessing camouflaging behaviors, further research involving more diverse, general population samples—ideally with clinical assessments—is needed. Furthermore, validating the instrument in clinical settings, particularly with individuals who have a confirmed autism diagnosis, is essential for ensuring its applicability in these contexts.
It is also important to consider that the self-report nature of the CAT-Q relies on individuals’ self-reflection and their ability to articulate their camouflaging behaviors and motivations. As a result, its applicability may be limited for those who have difficulty reflecting on their behaviors or expressing their motivations, such as some autistic individuals with language or intellectual challenges. To address this limitation, the CAT-Q can be supplemented with behavioral observations or informant-report measures of camouflaging. This combined approach allows for the assessment of camouflaging behaviors in individuals with limited self-insight or C abilities. By integrating the CAT-Q with observed behavioral and cognitive measures, a more comprehensive evaluation of this complex phenomenon can be achieved.
In the present study, given that group classification was based on AQ cut-offs, the high-AT group was comparatively smaller (n=52). This distribution is expected in community-based samples. Nonetheless, the total sample size (n=350) was sufficient for the psychometric analyses conducted.
Conclusion
The CAT-Q demonstrates its reliability and validity as an effective instrument for assessing social camouflaging behaviors. It shows considerable potential as a valuable tool for future research within Iranian populations, contributing to a better understanding of how social camouflaging manifests in this context. The CAT-Q’s ability to provide both theoretical and practical insights makes it a crucial tool for advancing research on social camouflaging, highlighting its importance for future studies in this field.
Ethical Considerations
Compliance with ethical guidelines
All research procedures were conducted in accordance with the ethical standards outlined in the 2013 Declaration of Helsinki. This study was approved by the Research Ethics Committee of the University of Mohaghegh Ardabili, Ardabil, Iran (Code: IR.UMA.REC.1403.052). Participation was fully voluntary, with written consent obtained from parents or legal guardians, alongside assent from the adolescent participants prior to data collection.
Funding
This study was extracted from the PhD dissertation of Sahar Khoshsorour, approved by the Department of Psychology, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran. This research did not receive any specific funding from public, commercial, or non-profit sector funding agencies.
Authors contributions
Data collection, statistical analyses, and writing the original draft: Sahar Khoshsorour; Review and editing: Mohammad Narimani and Sajjad Beshrpour; Conceptualization, methodology, and final approval: All authors; Supervision: Mohammad Narimani.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors gratefully acknowledge all the participants who generously dedicated their time and effort to complete the questionnaires for this study. Their valuable contributions have been instrumental in advancing our understanding of this field. The authors also extend their appreciation to the Education Departments of Districts 2, 5, and 6 of Tehran, who facilitated the recruitment of participants and supported the data collection process.
References
- Sasson NJ, Lam KS, Childress D, Parlier M, Daniels JL, Piven J. The B road A utism P henotype Q uestionnaire: Prevalence and Diagnostic Classification. Autism Res. 2013; 6(2):134-43. [DOI:10.1002/aur.1272] [PMID]
- Hannant P, Cassidy S, Tavassoli T, Mann F. Sensorimotor difficulties are associated with the severity of autism spectrum conditions. Front Integr Neurosci. 2016; 10:28. [DOI:10.3389/fnint.2016.00028] [PMID]
- Wigham S, Rodgers J, Berney T, Le Couteur A, Ingham B, Parr JR. Psychometric properties of questionnaires and diagnostic measures for autism spectrum disorders in adults: A systematic review. Autism. 2019; 23(2):287-305. [DOI:10.1177/1362361317748245] [PMID]
- Au-Yeung SK, Bradley L, Robertson AE, Shaw R, Baron-Cohen S, Cassidy S. Experience of mental health diagnosis and perceived misdiagnosis in autistic, possibly autistic and non-autistic adults. Autism. 2019; 23(6):1508-18.[DOI:10.1177/1362361318818167] [PMID]
- Werling DM, Geschwind DH. Sex differences in autism spectrum disorders. Curr Opin Neurol. 2013; 26(2):146-53. [DOI:10.1097/wco.0b013e32835ee548] [PMID]
- Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J, Warren Z, et al. Prevalence of Autism Spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 Sites, United States, 2014. MMWR Surveill Summ. 2018; 67(6):1-23. [DOI:10.15585/mmwr.ss6706a1] [PMID]
- Kirkovski M, Enticott PG, Fitzgerald PB. A review of the role of female gender in autism spectrum disorders. J Autism Dev Disord. 2013; 43(11):2584-603. [DOI:10.1007/s10803-013-1811-1] [PMID]
- Kreiser NL, White SW. ASD in females: Are we overstating the gender difference in diagnosis?. Clin Child Fam Psychol Rev. 2014; 17(1):67-84. [DOI:10.1007/s10567-013-0148-9] [PMID]
- Hull L, Petrides KV, Allison C, Smith P, Baron-Cohen S, Lai MC, et al. "Putting on My Best Normal": Social camouflaging in adults with autism spectrum conditions. J Autism Dev Disord. 2017; 47(8):2519-34. [DOI:10.1007/s10803-017-3166-5] [PMID]
- Zeldovich L. New global diagnostic criteria manual mirrors US autism criteria [Internet]. 2017 [Updated 2025 October 4]. Available from: [Link]
- Lai MC, Lombardo MV, Pasco G, Ruigrok AN, Wheelwright SJ, Sadek SA, et al. A behavioral comparison of male and female adults with high functioning autism spectrum conditions. PLoS One. 2011; 6(6):e20835. [DOI:10.1371/journal.pone.0020835] [PMID]
- Marazziti D, Abelli M, Baroni S, Carpita B, Piccinni A, Dell’Osso L. Recent findings on the pathophysiology of social anxiety disorder. Clinical Neuropsychiatry. 2014; 11(2). [Link]
- Dell’Osso L, Lorenzi P, Carpita B. Camouflaging: Psychopathological meanings and clinical relevance in autism spectrum conditions. CNS Spectr. 2021; 26(5):437-9. [DOI:10.1017/S1092852920001467] [PMID]
- Livingston LA, Happé F. Conceptualising compensation in neurodevelopmental disorders: Reflections from autism spectrum disorder. Neurosci Biobehav Rev. 2017; 80:729-42. [DOI:10.1016/j.neubiorev.2017.06.005] [PMID]
- Hull L, Mandy W, Lai MC, Baron-Cohen S, Allison C, Smith P, et al. Development and validation of the camouflaging autistic traits questionnaire (CAT-Q). J Autism Dev Disord. 2019; 49(3):819-33. [DOI:10.1007/s10803-018-3792-6] [PMID]
- Cage E, Troxell-Whitman Z. Understanding the reasons, contexts and costs of camouflaging for autistic adults. J Autism Dev Disord. 2019; 49(5):1899-911. [DOI:10.1007/s10803-018-03878-x] [PMID]
- Hull L, Lai MC, Baron-Cohen S, Allison C, Smith P, Petrides KV, et al. Gender differences in self-reported camouflaging in autistic and non-autistic adults. Autism. 2020; 24(2):352-63. [DOI:10.1177/1362361319864804] [PMID]
- Cage E, Di Monaco J, Newell V. Understanding, attitudes and dehumanisation towards autistic people. Autism. 2019; 23(6):1373-83. [DOI:10.1177/1362361318811290] [PMID]
- Bargiela S, Steward R, Mandy W. The experiences of late-diagnosed women with autism spectrum conditions: An investigation of the female autism phenotype. J Autism Dev Disord. 2016; 46(10):3281-94. [DOI:10.1007/s10803-016-2872-8] [PMID]
- Cassidy S, Bradley L, Shaw R, Baron-Cohen S. Risk markers for suicidality in autistic adults. Mol Autism. 2018; 9:42. [DOI:10.1186/s13229-018-0226-4] [PMID]
- Carpita B, Muti D, Petrucci A, Romeo F, Gesi C, Marazziti D, et al. Overlapping features between social anxiety and obsessive-compulsive spectrum in a clinical sample and in healthy controls: Toward an integrative model. CNS Spectr. 2020; 25(4):527-34. [DOI:10.1017/S109285291900138X] [PMID]
- Hull L, Petrides KV, Mandy W. Cognitive predictors of self‐reported camouflaging in autistic adolescents. Autism Res. 2021; 14(3):523-32. [DOI:10.1002/aur.2407] [PMID]
- Jung S, Lee S. Exploratory factor analysis for small samples. Behav Res Methods. 2011; 43(3):701-9. [DOI:10.3758/s13428-011-0077-9] [PMID]
- DeVellis RF, Thorpe CT. Scale development: Theory and applications. California: Sage Publications; 2021. [Link]
- Furr RM. Psychometrics: An introduction. California: SAGE Publications; 2021. [Link]
- La Greca AM, Lopez N. Social anxiety among adolescents: linkages with peer relations and friendships. J Abnorm Child Psychol. 1998; 26(2):83-94. [DOI:10.1023/A:1022684520514] [PMID]
- Vernberg EM, Abwender DA, Ewell KK, Beery SH. Social anxiety and peer relationships in early adolescence: A prospective analysis. J Clin Child Psychol. 1992; 21(2):189-96. [DOI:10.1207/s15374424jccp2102_11]
- Inderbitzen-Nolan HM, Walters KS. Social anxiety scale for adolescents: Normative data and further evidence of construct validity. J Clin Child Psychol. 2000; 29(3):360-71. [DOI:10.1207/S15374424JCCP2903_7] [PMID]
- Ostvar S, Razavieh A. [The study of psychometric properties of social anxiety Scale For Adolescents (Sas-A) for use In Iran (Persian)]. J Psychol Model Methods. 2013; 3(12):69-78. [Link]
- Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The autism-spectrum quotient (AQ): Evidence from asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord. 2001; 31(1):5-17. [DOI:10.1023/A:1005653411471] [PMID]
- Nejati Safa AA, Kazemi MR, Alaghband Rad J. [Autistic Features in Adult Population: Evidence for continuity of autistic symptoms with normality (Persian)]. Adv Cogn Sci. 2003; 5(3):34-9. [Link]
- Robertson AE, Simmons DR. The relationship between sensory sensitivity and autistic traits in the general population. J Autism Dev Disord. 2013; 43(4):775-84. [DOI:10.1007/s10803-012-1608-7] [PMID]
- Lei J, Leigh E, Charman T, Russell A, Hollocks MJ. Understanding the relationship between social camouflaging in autism and safety behaviours in social anxiety in autistic and non-autistic adolescents. J Child Psychol Psychiatry. 2024; 65(3):285-97. [DOI:10.1111/jcpp.13884] [PMID]
- Tierney S, Burns J, Kilbey E. Looking behind the mask: Social coping strategies of girls on the autistic spectrum. Res Autism Spectr Disord. 2016; 23:73-83. [DOI:10.1016/j.rasd.2015.11.013]
- Hull L, Petrides KV, Mandy W. The female autism phenotype and camouflaging: A narrative review. Rev J Autism Dev Disord. 2020; 7:306-17. [DOI:10.1007/s40489-020-00197-9]
- Dell'Osso L, Cremone IM, Muti D, Massimetti G, Lorenzi P, Carmassi C, et al. Validation of the Italian version of the Camouflaging Autistic Traits Questionnaire (CAT-Q) in a University population. Compr Psychiatry. 2022; 114:152295. [DOI:10.1016/j.comppsych.2022.152295] [PMID]
- Bureau R, Riebel M, Weiner L, Coutelle R, Dachez J, Clément C. French Validation of the Camouflaging Autistic Traits Questionnaire (CAT-Q). J Autism Dev Disord. 2024; 54(9):3549-58. [DOI:10.1007/s10803-023-06048-w] [PMID]
- van der Putten WJ, van Rentergem JA, Radhoe TA, Torenvliet C, Groenman AP, Mol AJ, et al. How to measure camouflaging? A conceptual replication of the validation of the Camouflaging Autistic Traits Questionnaire in Dutch adults. Res Autism Spectr Disord. 2023; 100:102072. [DOI:10.1016/j.rasd.2022.102072]
- Hongo M, Oshima F, Guan S, Takahashi T, Nitta Y, Seto M, et al. Reliability and validity of the Japanese version of the camouflaging autistic traits questionnaire. Autism Res. 2024; 17(6):1205-17. [DOI:10.1002/aur.3137] [PMID]
- Liu CH, Chen YL, Chen PJ, Ni HC, Lai MC. Exploring camouflaging by the Chinese version Camouflaging Autistic Traits Questionnaire in Taiwanese autistic and non-autistic adolescents: An initial development. Autism. 2024; 28(3):690-704. [DOI:10.1177/13623613231181732] [PMID]
Type of Study: Research |
Subject:
Special
Received: 2024/10/5 | Accepted: 2025/07/26 | Published: 2025/10/26
Received: 2024/10/5 | Accepted: 2025/07/26 | Published: 2025/10/26
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
