Fri, Jan 2, 2026
Volume 11, Issue 2 (Spring 2025)
Caspian J Neurol Sci 2025, 11(2): 163-171 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dehnavi M, Jafarnejadgero A, Tabatabai Ghomsheh F, Fattahi A. The Effect of Eight Weeks of Strength and Balance Training on Kinetic Variables in Elderly. Caspian J Neurol Sci 2025; 11 (2) :163-171
URL: http://cjns.gums.ac.ir/article-1-746-en.html
URL: http://cjns.gums.ac.ir/article-1-746-en.html



1- Department of Sports Biomechanics, Faculty of Sport Science and Physical Education, Central Tehran Branch, Islamic Azad University, Tehran, Iran. , mahboobeh.dehnavi@gmail.com
2- Department of Sport Biomechanics, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
3- Department of Ergonomics, Pediatric Neurorehabilitation Research Center, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences (USWR), Tehran, Iran.
4- Department of Sports Biomechanics, Faculty of Sport Science and Physical Education, Central Tehran Branch, Islamic Azad University, Tehran, Iran.
2- Department of Sport Biomechanics, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
3- Department of Ergonomics, Pediatric Neurorehabilitation Research Center, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences (USWR), Tehran, Iran.
4- Department of Sports Biomechanics, Faculty of Sport Science and Physical Education, Central Tehran Branch, Islamic Azad University, Tehran, Iran.
Full-Text [PDF 1314 kb]
(1162 Downloads)
| Abstract (HTML) (1134 Views)
Full-Text: (547 Views)
Introduction
The phenomenon of aging is one of the inevitable events that occurs with increasing age in human society [1]. The aging process is associated with extensive alterations and challenges within the peripheral, physical, and motor nervous systems, resulting in various forms of weakness. Notable musculoskeletal, vestibular, sensory and visual changes contribute to these declines [2]. The most common changes and problems among older people are fear of falling, balance disorder, decreased muscle strength, vision problems, taking multiple drugs (defined as taking more than four drugs), difficulty walking, depression, and functional limitations [3]. Statistically, more than 30% of people over 60 fall every year. In almost half of the cases, the history of falls is repeated [4]. Among the stated problems, balance and postural control are essential for these people.
Postural control includes controlling the body’s position in space for the two purposes of stability and orientation. In old age, losing balance is a constant concern, especially with increasing age. Balance impairment is a strong risk factor for falls in older people [5]. In this regard, studies have investigated the effect of various exercises, such as pilates exercises [6], visual feedback [7], exergame exercises [8] and multicomponent exercises [9], on the balance and postural control of older people. The results of their studies showed that exercises have a positive effect on the mentioned factors. Despite the impact of exercises on improving balance, it is still reported that the fall rate of older people is high [10]. Among the studies conducted on the postural control of older people, studies have also investigated the effect of balance and strength training on the postural control of the elderly. Additionally, The results of studies show that balance training affects the postural control of older people [11, 12] and strength training has improved the postural control of older people [13, 14].
Balance training enhances the number of mechanoreceptors and improves neuromuscular coordination, enabling the central nervous system to activate muscle motor nerves in a precise and coordinated manner. All these factors improve a person’s balance while performing functional activities [15]. The increase in balance as a result of strength training can be the result of increasing the muscle strength of the subjects’ lower limbs after participating in the training program, facilitating the activation of fast-twitch and large motor units, increasing muscle coordination, and exerting pressure on the neuromuscular systems [16].
By reviewing the studies, it is clear that exercise has a positive effect on the postural control of older people. However, studies have not investigated and compared these two types of balance and strength training to determine which is more effective in controlling the postural of older people. The comparison of balance and strength training is vital for older people. First, it enhances understanding of how these exercise modalities affect the neuromuscular system, with balance training focusing on mechanoreceptor sensitivity and coordination, while strength training emphasizes muscle power. Second, these training types are complementary; balance training improves joint awareness and coordination, while strength training boosts muscle strength and efficiency, creating a synergistic effect that maximizes functional performance and reduces fall risk. Third, this knowledge enables healthcare professionals to tailor rehabilitation programs to the specific needs of older adults, ensuring that those with strength deficits benefit from strength training and those with coordination issues engage in balance-focused exercises. Therefore, this study aims to compare the effect of strength and balance training on the kinetic variables of healthy older people.
Materials and Methods
Considering the application of the intervention variable (strength and balance training) and the random selection of the participants from society, the current research was quasi-experimental in terms of method and strategy. In terms of the topic, research was applied with a pre-test-post-test design. Participants in this study were randomly assigned into 3 parallel arms, including the balance training group (n=12), strength training group (n=12), and control group (n=12). The control group did not engage in any exercise or training programs and continued with their regular daily activities. The statistical population of this research consisted of healthy older people from Tehran City, Iran, within an age range of 60 to 75 years. The results of similar previous studies [17] and G*Power software, version 3.1.9.7 were used to determine the sample size. Based on this information, the number of samples in each group was calculated with a confidence interval (CI) of 0.95, a test power of 80% and an effect size of 0.5. With the possible loss of samples, three participants, more than calculated by the software, were considered in each group. It should be noted that to estimate the sample size, the reported effect size was used concerning the balance indices. The statistical sample of this research included 36 participants (12 participants in each group) with an age range of 60 to 75 years.
The inclusion criteria of the research include being female, being at least 60 years old and at most 74 years old (young elderly), lacking cardiovascular and respiratory diseases, having no record of falling in the last six months, getting a score of 24 or higher in the mini-mental state test (MMSE), giving written consent to participate, avoiding sports exercises or intense activities during the research, the absence of postural abnormalities affecting the research process (in the lower and upper limbs) and having the commitments of the physical activity readiness questionnaire and the subjects’ health questionnaire. The exclusion criteria during the research were failure to participate in two consecutive training sessions or three non-consecutive training sessions and the occurrence of musculoskeletal pain after performing the training.
A height-measuring device was used to measure the height of the participants. A digital scale measured the subjects’ weight with an accuracy of 100 g without shoes and with minimal clothing. The age of the participants was also recorded based on the age of the birth certificate of the participants.
Cognitive status test
The MMSE test is used in many parts of the world and different cultures due to its ability to execute well. It provides a general estimate of a person’s mental state by measuring different cognitive functions. Despite some restrictions, this test has also been translated into various languages and its use is still widespread among illiterate people. It has 20 questions, consists of four scales (locating, recording, paying attention, and calculating and recalling) and has a total score of 30 points. A score between 24 and 30 indicates cognitive health and a score of 23 or lower indicates cognitive impairment. Thus, a score of 21 to 23 indicates mild cognitive impairment, 10 to 21 indicates moderate cognitive impairment and a score below 9 indicates severe cognitive impairment. Trzepacz and Hochstetler measured this questionnaire with good validity and reliability, which has been confirmed through Cronbach α [18].
Evaluate kinetic variables
Sways of the center of pressure include the measurement of the indices of postural sways, Mean±SD speed in the anterior-posterior (AP) and mediolateral (ML) direction, and the sway area (95% CI). It was measured by force plate Kistler (Kistler) model 9286B (made in Switzerland), with a frequency of 1000 Hz. The average of three measured repetitions of the mentioned indicators was calculated. The sway area was calculated using MATLAB software, version R2024b. To remove possible noises, all the data were filtered using a 20-degree low-pass Butterworth filter [19].
The participant stands on two legs on a stable surface with eyes open and without sensory interference. The hands of the participants were placed on the waist. Each participant performed the test for 30 seconds [20]. During the assessment, participants were instructed to adopt a neutral stance with feet shoulder-width apart and were given clear verbal instructions on maintaining their balance. Also, participants performed the balance assessments on the force plate while barefoot.
Balance training program
The training program for the balance training group was applied regarding Martínez-Amat et al. [21], Clark and Burden [22] and Carmeli et al. [23] recommendations. To perform balance training, the participants attended the training hall for 8 weeks (three sessions per week on odd days) from 10 to 11 AM. Each training session lasted 60 minutes (5 minutes of warming up, 50 minutes of training protocol, and 5 minutes of cooling down). Table 1 presents the training protocol and the progress of the training protocol during the coming weeks.

Strength training program
The participants attended the training hall for 8 weeks (three sessions per week on even days) to perform strength training from 10 to 11 AM. Each training session lasted 60 minutes (5 minutes of warming up, 50 minutes of training protocol, and 5 minutes of cooling down). Strength training consisted of performing a set of 12 repetitions of exercises for 8 muscle groups (quadriceps muscles, hip adductor muscles, hip abductor muscles, gluteal muscles, hamstring muscles, leg muscles, pectoral muscles and back muscles). The intensity of the exercises and the volume of weights according to the age and ability of older people and according to the target muscle were considered from 35% to 65% of a maximum repetition. Gradually, when the participants could perform more than the repetitions determined in each given intensity, the volume of weights increased. Finally, 10 minutes of cooling was done [24]. However, we provided a clear explanation of determining 1RM in this population, recognizing that traditional 1RM testing posed risks for older adults. To enhance safety, we considered using submaximal testing methods, such as the multiple-repetition maximum (e.g. 5-10 reps) or perceived exertion scales to estimate strength levels. Additionally, we included precautions such as ensuring proper warm-up, using supportive equipment, and having trained personnel present during testing to monitor form and provide assistance if needed. This approach helped minimize risks while still accurately assessing strength capabilities in elderly individuals.
Statistical analysis
In this research, descriptive statistics are used to describe the data of each group (age, height, leg length, subjects’ weight, body mass index). Mean±SD index were used to describe the data. The normality of all data before and after interventions was checked with the Shapiro-Wilk test. Levene’s test was used to check the homogeneity of variances. Analysis of covariance was used to compare the average pre-test and post-test data of the experimental and control groups. Comparison of the results of each parameter using two-factor mixed measurement analysis of variance tests with an intra-group variable of time (pre-test-post-test) and an inter-group variable of location (groups 1, 2 and control group), and Bonferroni post hoc test was performed at a significance level of P<0.05. Statistical software SPSS software, version 28 and Excel software, version 2019 were used for statistical calculations and graph drawing. Also, standard effect sizes were used to investigate the effect sizes of training protocols on postural control [25]. In the standard method, the effect sizes are divided into three parts: Small (0.02), medium (0.05), and large (0.8 and above). Also, all desired variables were calculated with a 95% CI.
Results
Table 2 presents the groups’ Mean±SD of demographic data (age, height and weight).
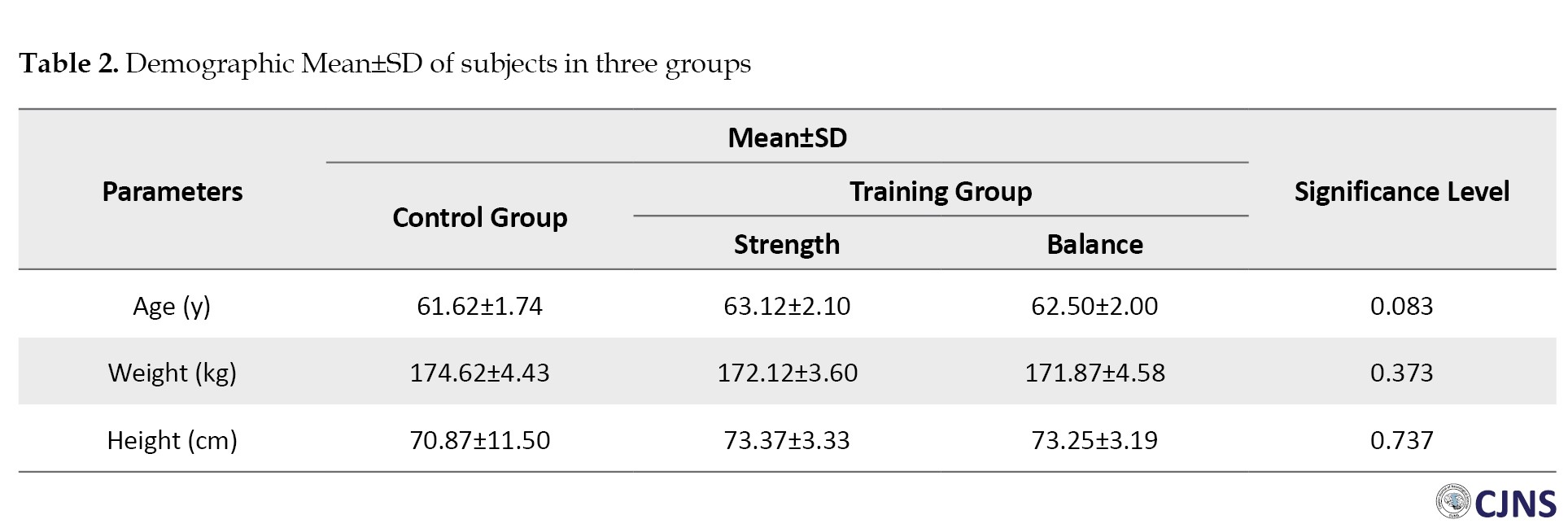
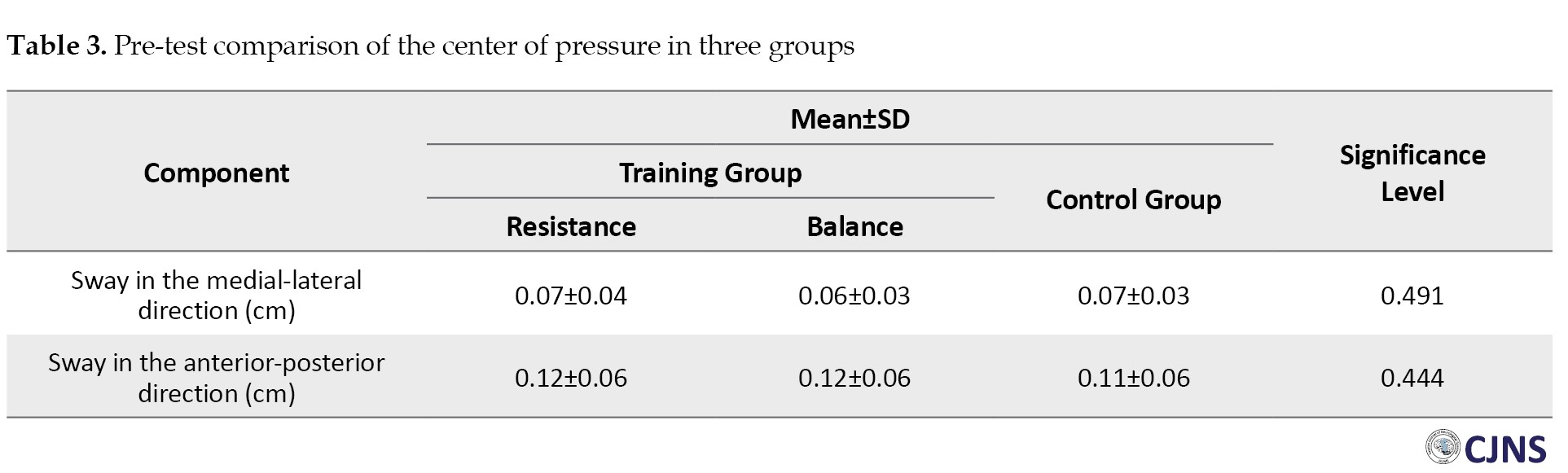
The results showed no statistically significant difference between the subjects’ average height, weight and age in the three groups. According to the obtained results, none of the components of the center of pressure in the pre-test stage between the three groups were significant (P<0.05) (Table 3).
The effect of the time factor in the changes of the center of pressure in the AP direction had a statistically significant difference (P=0.031; d=0.211). No statistically significant difference was observed in other components (P<0.05) (Table 4).
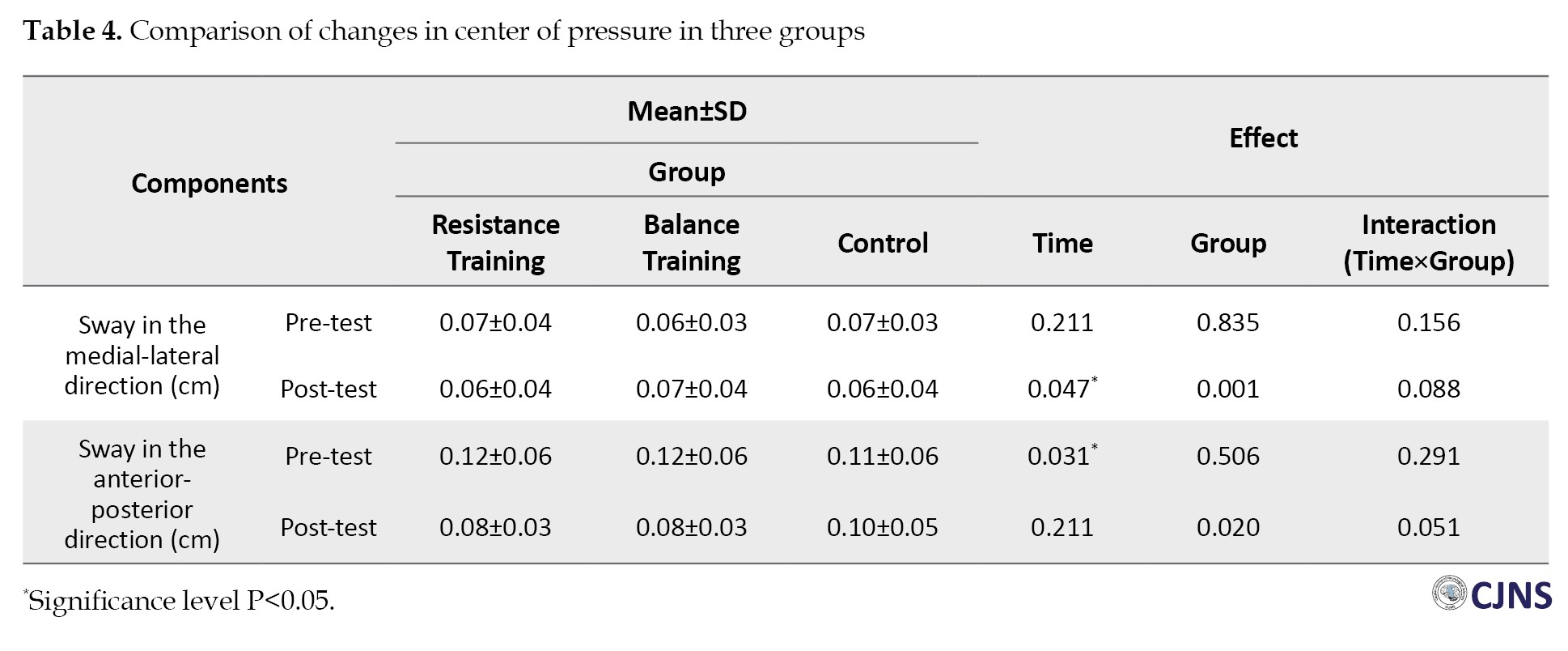
Therefore, the Bonferroni post hoc test was used to detect group differences.
According to the results of Table 5, the Bonferroni post hoc test shows a significant difference in the average sways in the medial-lateral and AP directions between the balance and strength exercises-control groups in the post-test.
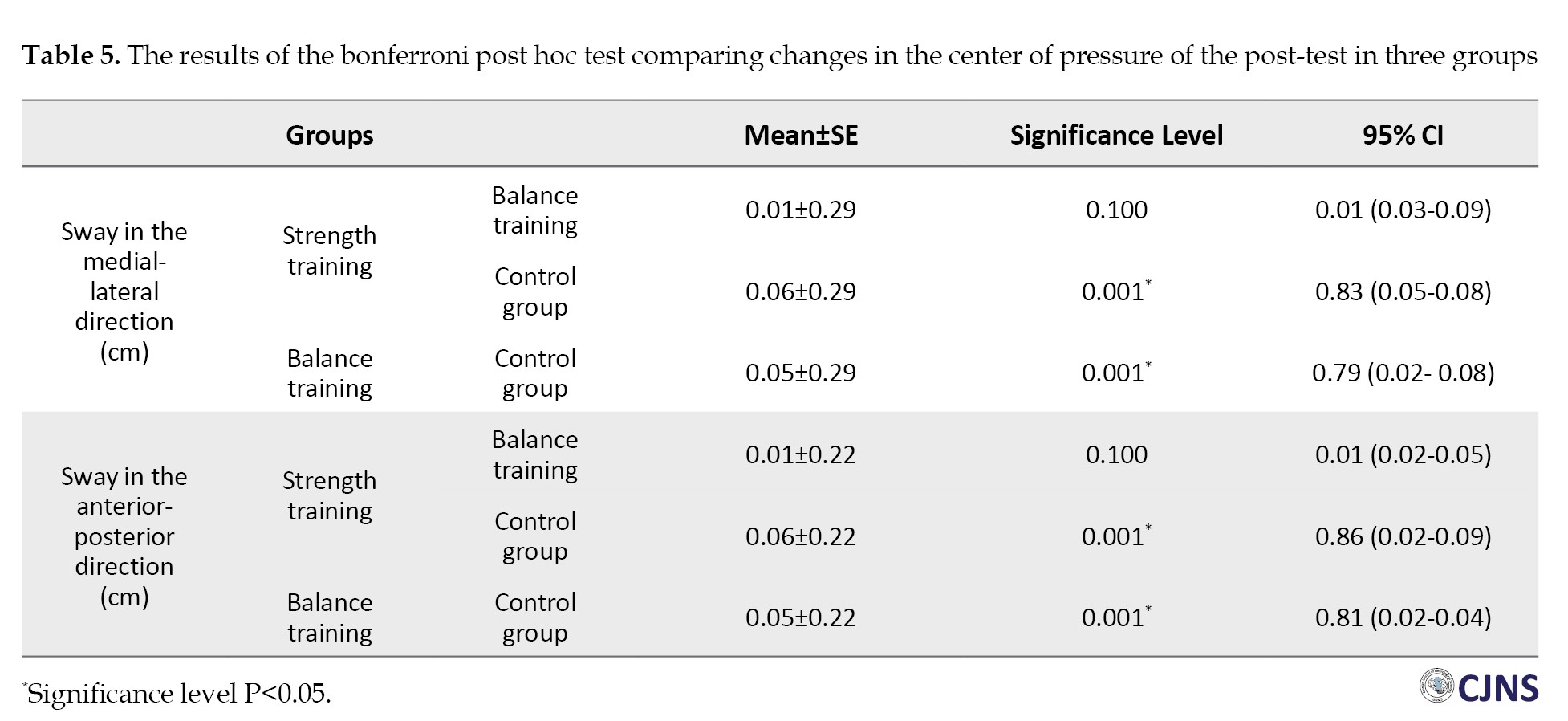
However, the Bonferroni post hoc test does not show a significant difference in the average sways in the medial-lateral and AP directions between the groups of strength-balance exercises.
Discussion
This study aimed to investigate the effect of 8 weeks of strength and balance training on the kinetic variables of healthy older people. The results of the study showed that both balance and strength training have a significant effect on the kinetic variables of older people. Also, the research results showed no significant difference between strength and balance training on the kinetic variables of older people. Therefore, it seems that balance and strength training significantly affect the postural control of older people.
The results of the present study on the effect of balance and strength training on the postural control of older people are consistent with the results of the studies of Casonatto and Yamacita [26], Shahrbanian et al. [27]. These studies showed that exercise programs improve postural control in older people. The exercise program that is applied to the postural control of older people seems to improve their postural control. One of the reasons for the improvement of postural control due to exercise protocols can be considered the effect of mobility because of lack of participation in sports activities due to isolationism; escaping from normal populations can also be considered one of the causes of low postural control in older people, which has caused participation in any exercise program. The intervention of any exercise protocol positively affects the postural control of older people, which affects their mobility.
Balance training on unbalanced surfaces enhances nerve conduction speed, muscle coordination and muscle fibers’ adaptability while stimulating mechanoreceptors in the skin and joints. Effective balance requires motor control responses from the brain stem, spinal cord reflexes, and cortex-conscious responses. This training improves postural control by stimulating the central nervous system, which coordinates agonist and antagonist muscles, which are crucial for stabilizing lower limb joints [28].
The motion control system’s inputs and outputs are closely interconnected, meaning that changes in sensory inputs can significantly impact movement performance. Improvements in postural control may stem from enhanced neuromuscular adaptations due to training, such as the recruitment of more efficient nerve units, reorganization in the sensory-motor cortex, strengthened synaptic connections, increased nervous system activation, and reduced inhibitory reflexes. Neurologically, this includes decreased resistance along neural pathways, facilitating the transmission of sensory inputs from the body [29]. In this way, it seems that balance training, while increasing the accuracy of joint proprioception, also affects the outputs of the postural control system. Reducing the number of sways, the speed of sways, and the sway area in the subjects’ kinetic patterns within the range of the support level plays an essential role in improving their postural control.
Strength training significantly impacts the postural control of older people by enhancing neuromuscular control. After strength training, individuals can effectively recruit the necessary motor units and muscle fibers, resulting in increased nerve stimulation to the lower limb muscles [30]. This heightened awareness of muscle function, trunk control, and hip positioning contributes to greater force production in the lower limbs. Improved force output is crucial for maintaining better postural control, as muscle strength is key in preventing postural sway among older people [31]. Conversely, decreased muscle strength disrupts postural control and is a significant health concern, often leading to a higher risk of falls [32]. Therefore, enhancing lower limb strength in older adults is essential for improving their balance and overall postural stability, as there is a strong correlation between reduced muscle strength and poor postural control in this population [33].
Strength training can enhance force and power output by reducing the inhibitory effects of golgi tendon receptors, which limits force production. These receptors act as tension regulators, and their sensitivity can hinder muscle performance. Strength training decreases this sensitivity, allowing greater force generation as more load is applied to the muscles [34]. Additionally, neuromuscular coordination plays a crucial role in improving power output. The speed of muscle contraction relies on effective coordination, and strength training fosters neuromuscular adaptations that enhance muscle performance, mainly through explosive movements [35]. Together, these mechanisms contribute to better postural control in older people.
Conclusion
The present study showed that balance and strength training significantly affect the postural control of older people. Also, the research results showed no significant difference between balance and strength training in the postural control of older people. Therefore, balance and strength training can be used as alternatives to improve the postural control of the elderly and thus reduce the risk of falls in older people.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Sari branch, Sari, Iran (Code: IR.IAU.SARI.REC.1403.109). All experiments were performed in accordance with relevant guidelines and regulations.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Methodology: Mahboobeh Dehnavi and Amirali Jafarnejadgero; Investigation and funding acquisition: Mahboobeh Dehnavi; Supervision: Amirali Jafarnejadgero, Farhad Tabatabai Ghomsheh and Ali Fattahi; Conceptualization, resources, writing the original draft, writing, review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The researchers would like to express gratitude towards all the participants who contributed to conducting the study.
References
The phenomenon of aging is one of the inevitable events that occurs with increasing age in human society [1]. The aging process is associated with extensive alterations and challenges within the peripheral, physical, and motor nervous systems, resulting in various forms of weakness. Notable musculoskeletal, vestibular, sensory and visual changes contribute to these declines [2]. The most common changes and problems among older people are fear of falling, balance disorder, decreased muscle strength, vision problems, taking multiple drugs (defined as taking more than four drugs), difficulty walking, depression, and functional limitations [3]. Statistically, more than 30% of people over 60 fall every year. In almost half of the cases, the history of falls is repeated [4]. Among the stated problems, balance and postural control are essential for these people.
Postural control includes controlling the body’s position in space for the two purposes of stability and orientation. In old age, losing balance is a constant concern, especially with increasing age. Balance impairment is a strong risk factor for falls in older people [5]. In this regard, studies have investigated the effect of various exercises, such as pilates exercises [6], visual feedback [7], exergame exercises [8] and multicomponent exercises [9], on the balance and postural control of older people. The results of their studies showed that exercises have a positive effect on the mentioned factors. Despite the impact of exercises on improving balance, it is still reported that the fall rate of older people is high [10]. Among the studies conducted on the postural control of older people, studies have also investigated the effect of balance and strength training on the postural control of the elderly. Additionally, The results of studies show that balance training affects the postural control of older people [11, 12] and strength training has improved the postural control of older people [13, 14].
Balance training enhances the number of mechanoreceptors and improves neuromuscular coordination, enabling the central nervous system to activate muscle motor nerves in a precise and coordinated manner. All these factors improve a person’s balance while performing functional activities [15]. The increase in balance as a result of strength training can be the result of increasing the muscle strength of the subjects’ lower limbs after participating in the training program, facilitating the activation of fast-twitch and large motor units, increasing muscle coordination, and exerting pressure on the neuromuscular systems [16].
By reviewing the studies, it is clear that exercise has a positive effect on the postural control of older people. However, studies have not investigated and compared these two types of balance and strength training to determine which is more effective in controlling the postural of older people. The comparison of balance and strength training is vital for older people. First, it enhances understanding of how these exercise modalities affect the neuromuscular system, with balance training focusing on mechanoreceptor sensitivity and coordination, while strength training emphasizes muscle power. Second, these training types are complementary; balance training improves joint awareness and coordination, while strength training boosts muscle strength and efficiency, creating a synergistic effect that maximizes functional performance and reduces fall risk. Third, this knowledge enables healthcare professionals to tailor rehabilitation programs to the specific needs of older adults, ensuring that those with strength deficits benefit from strength training and those with coordination issues engage in balance-focused exercises. Therefore, this study aims to compare the effect of strength and balance training on the kinetic variables of healthy older people.
Materials and Methods
Considering the application of the intervention variable (strength and balance training) and the random selection of the participants from society, the current research was quasi-experimental in terms of method and strategy. In terms of the topic, research was applied with a pre-test-post-test design. Participants in this study were randomly assigned into 3 parallel arms, including the balance training group (n=12), strength training group (n=12), and control group (n=12). The control group did not engage in any exercise or training programs and continued with their regular daily activities. The statistical population of this research consisted of healthy older people from Tehran City, Iran, within an age range of 60 to 75 years. The results of similar previous studies [17] and G*Power software, version 3.1.9.7 were used to determine the sample size. Based on this information, the number of samples in each group was calculated with a confidence interval (CI) of 0.95, a test power of 80% and an effect size of 0.5. With the possible loss of samples, three participants, more than calculated by the software, were considered in each group. It should be noted that to estimate the sample size, the reported effect size was used concerning the balance indices. The statistical sample of this research included 36 participants (12 participants in each group) with an age range of 60 to 75 years.
The inclusion criteria of the research include being female, being at least 60 years old and at most 74 years old (young elderly), lacking cardiovascular and respiratory diseases, having no record of falling in the last six months, getting a score of 24 or higher in the mini-mental state test (MMSE), giving written consent to participate, avoiding sports exercises or intense activities during the research, the absence of postural abnormalities affecting the research process (in the lower and upper limbs) and having the commitments of the physical activity readiness questionnaire and the subjects’ health questionnaire. The exclusion criteria during the research were failure to participate in two consecutive training sessions or three non-consecutive training sessions and the occurrence of musculoskeletal pain after performing the training.
A height-measuring device was used to measure the height of the participants. A digital scale measured the subjects’ weight with an accuracy of 100 g without shoes and with minimal clothing. The age of the participants was also recorded based on the age of the birth certificate of the participants.
Cognitive status test
The MMSE test is used in many parts of the world and different cultures due to its ability to execute well. It provides a general estimate of a person’s mental state by measuring different cognitive functions. Despite some restrictions, this test has also been translated into various languages and its use is still widespread among illiterate people. It has 20 questions, consists of four scales (locating, recording, paying attention, and calculating and recalling) and has a total score of 30 points. A score between 24 and 30 indicates cognitive health and a score of 23 or lower indicates cognitive impairment. Thus, a score of 21 to 23 indicates mild cognitive impairment, 10 to 21 indicates moderate cognitive impairment and a score below 9 indicates severe cognitive impairment. Trzepacz and Hochstetler measured this questionnaire with good validity and reliability, which has been confirmed through Cronbach α [18].
Evaluate kinetic variables
Sways of the center of pressure include the measurement of the indices of postural sways, Mean±SD speed in the anterior-posterior (AP) and mediolateral (ML) direction, and the sway area (95% CI). It was measured by force plate Kistler (Kistler) model 9286B (made in Switzerland), with a frequency of 1000 Hz. The average of three measured repetitions of the mentioned indicators was calculated. The sway area was calculated using MATLAB software, version R2024b. To remove possible noises, all the data were filtered using a 20-degree low-pass Butterworth filter [19].
The participant stands on two legs on a stable surface with eyes open and without sensory interference. The hands of the participants were placed on the waist. Each participant performed the test for 30 seconds [20]. During the assessment, participants were instructed to adopt a neutral stance with feet shoulder-width apart and were given clear verbal instructions on maintaining their balance. Also, participants performed the balance assessments on the force plate while barefoot.
Balance training program
The training program for the balance training group was applied regarding Martínez-Amat et al. [21], Clark and Burden [22] and Carmeli et al. [23] recommendations. To perform balance training, the participants attended the training hall for 8 weeks (three sessions per week on odd days) from 10 to 11 AM. Each training session lasted 60 minutes (5 minutes of warming up, 50 minutes of training protocol, and 5 minutes of cooling down). Table 1 presents the training protocol and the progress of the training protocol during the coming weeks.
Strength training program
The participants attended the training hall for 8 weeks (three sessions per week on even days) to perform strength training from 10 to 11 AM. Each training session lasted 60 minutes (5 minutes of warming up, 50 minutes of training protocol, and 5 minutes of cooling down). Strength training consisted of performing a set of 12 repetitions of exercises for 8 muscle groups (quadriceps muscles, hip adductor muscles, hip abductor muscles, gluteal muscles, hamstring muscles, leg muscles, pectoral muscles and back muscles). The intensity of the exercises and the volume of weights according to the age and ability of older people and according to the target muscle were considered from 35% to 65% of a maximum repetition. Gradually, when the participants could perform more than the repetitions determined in each given intensity, the volume of weights increased. Finally, 10 minutes of cooling was done [24]. However, we provided a clear explanation of determining 1RM in this population, recognizing that traditional 1RM testing posed risks for older adults. To enhance safety, we considered using submaximal testing methods, such as the multiple-repetition maximum (e.g. 5-10 reps) or perceived exertion scales to estimate strength levels. Additionally, we included precautions such as ensuring proper warm-up, using supportive equipment, and having trained personnel present during testing to monitor form and provide assistance if needed. This approach helped minimize risks while still accurately assessing strength capabilities in elderly individuals.
Statistical analysis
In this research, descriptive statistics are used to describe the data of each group (age, height, leg length, subjects’ weight, body mass index). Mean±SD index were used to describe the data. The normality of all data before and after interventions was checked with the Shapiro-Wilk test. Levene’s test was used to check the homogeneity of variances. Analysis of covariance was used to compare the average pre-test and post-test data of the experimental and control groups. Comparison of the results of each parameter using two-factor mixed measurement analysis of variance tests with an intra-group variable of time (pre-test-post-test) and an inter-group variable of location (groups 1, 2 and control group), and Bonferroni post hoc test was performed at a significance level of P<0.05. Statistical software SPSS software, version 28 and Excel software, version 2019 were used for statistical calculations and graph drawing. Also, standard effect sizes were used to investigate the effect sizes of training protocols on postural control [25]. In the standard method, the effect sizes are divided into three parts: Small (0.02), medium (0.05), and large (0.8 and above). Also, all desired variables were calculated with a 95% CI.
Results
Table 2 presents the groups’ Mean±SD of demographic data (age, height and weight).
The results showed no statistically significant difference between the subjects’ average height, weight and age in the three groups. According to the obtained results, none of the components of the center of pressure in the pre-test stage between the three groups were significant (P<0.05) (Table 3).
The effect of the time factor in the changes of the center of pressure in the AP direction had a statistically significant difference (P=0.031; d=0.211). No statistically significant difference was observed in other components (P<0.05) (Table 4).
Therefore, the Bonferroni post hoc test was used to detect group differences.
According to the results of Table 5, the Bonferroni post hoc test shows a significant difference in the average sways in the medial-lateral and AP directions between the balance and strength exercises-control groups in the post-test.
However, the Bonferroni post hoc test does not show a significant difference in the average sways in the medial-lateral and AP directions between the groups of strength-balance exercises.
Discussion
This study aimed to investigate the effect of 8 weeks of strength and balance training on the kinetic variables of healthy older people. The results of the study showed that both balance and strength training have a significant effect on the kinetic variables of older people. Also, the research results showed no significant difference between strength and balance training on the kinetic variables of older people. Therefore, it seems that balance and strength training significantly affect the postural control of older people.
The results of the present study on the effect of balance and strength training on the postural control of older people are consistent with the results of the studies of Casonatto and Yamacita [26], Shahrbanian et al. [27]. These studies showed that exercise programs improve postural control in older people. The exercise program that is applied to the postural control of older people seems to improve their postural control. One of the reasons for the improvement of postural control due to exercise protocols can be considered the effect of mobility because of lack of participation in sports activities due to isolationism; escaping from normal populations can also be considered one of the causes of low postural control in older people, which has caused participation in any exercise program. The intervention of any exercise protocol positively affects the postural control of older people, which affects their mobility.
Balance training on unbalanced surfaces enhances nerve conduction speed, muscle coordination and muscle fibers’ adaptability while stimulating mechanoreceptors in the skin and joints. Effective balance requires motor control responses from the brain stem, spinal cord reflexes, and cortex-conscious responses. This training improves postural control by stimulating the central nervous system, which coordinates agonist and antagonist muscles, which are crucial for stabilizing lower limb joints [28].
The motion control system’s inputs and outputs are closely interconnected, meaning that changes in sensory inputs can significantly impact movement performance. Improvements in postural control may stem from enhanced neuromuscular adaptations due to training, such as the recruitment of more efficient nerve units, reorganization in the sensory-motor cortex, strengthened synaptic connections, increased nervous system activation, and reduced inhibitory reflexes. Neurologically, this includes decreased resistance along neural pathways, facilitating the transmission of sensory inputs from the body [29]. In this way, it seems that balance training, while increasing the accuracy of joint proprioception, also affects the outputs of the postural control system. Reducing the number of sways, the speed of sways, and the sway area in the subjects’ kinetic patterns within the range of the support level plays an essential role in improving their postural control.
Strength training significantly impacts the postural control of older people by enhancing neuromuscular control. After strength training, individuals can effectively recruit the necessary motor units and muscle fibers, resulting in increased nerve stimulation to the lower limb muscles [30]. This heightened awareness of muscle function, trunk control, and hip positioning contributes to greater force production in the lower limbs. Improved force output is crucial for maintaining better postural control, as muscle strength is key in preventing postural sway among older people [31]. Conversely, decreased muscle strength disrupts postural control and is a significant health concern, often leading to a higher risk of falls [32]. Therefore, enhancing lower limb strength in older adults is essential for improving their balance and overall postural stability, as there is a strong correlation between reduced muscle strength and poor postural control in this population [33].
Strength training can enhance force and power output by reducing the inhibitory effects of golgi tendon receptors, which limits force production. These receptors act as tension regulators, and their sensitivity can hinder muscle performance. Strength training decreases this sensitivity, allowing greater force generation as more load is applied to the muscles [34]. Additionally, neuromuscular coordination plays a crucial role in improving power output. The speed of muscle contraction relies on effective coordination, and strength training fosters neuromuscular adaptations that enhance muscle performance, mainly through explosive movements [35]. Together, these mechanisms contribute to better postural control in older people.
Conclusion
The present study showed that balance and strength training significantly affect the postural control of older people. Also, the research results showed no significant difference between balance and strength training in the postural control of older people. Therefore, balance and strength training can be used as alternatives to improve the postural control of the elderly and thus reduce the risk of falls in older people.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Islamic Azad University, Sari branch, Sari, Iran (Code: IR.IAU.SARI.REC.1403.109). All experiments were performed in accordance with relevant guidelines and regulations.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Methodology: Mahboobeh Dehnavi and Amirali Jafarnejadgero; Investigation and funding acquisition: Mahboobeh Dehnavi; Supervision: Amirali Jafarnejadgero, Farhad Tabatabai Ghomsheh and Ali Fattahi; Conceptualization, resources, writing the original draft, writing, review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The researchers would like to express gratitude towards all the participants who contributed to conducting the study.
References
- Kiik SM, Vanchapo AR, Elfrida MF, Nuwa MS, Sakinah S. Effectiveness of otago exercise on health status and risk of fall among elderly with chronic illness. J Keperawatan Indones. 2020; 23(1):15-22. [DOI:10.7454/jki.v23i1.900]
- Wayne PM, Gow BJ, Hou F, Ma Y, Hausdorff JM, Lo J, et al. Tai Chi training's effect on lower extremity muscle co-contraction during single- and dual-task gait: Cross-sectional and randomized trial studies. Plos One. 2021; 16(1):e0242963.[DOI:10.1371/journal.pone.0242963] [PMID] [PMCID]
- Dudás V. A Comprehensive analysis of fall risk and prevention. Science Insights. 2024; 44(5):1365-73. [DOI:10.15354/si.24.re1002]
- Appeadu M, Bordoni B. Falls and fall prevention in older adults. Treasure Island: StatPearls; 2023. [Link]
- Osoba MY, Rao AK, Agrawal SK, Lalwani AK. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig Otolaryngol. 2019; 4(1):143-53. [DOI:10.1002/lio2.252] [PMID] [PMCID]
- Barker AL, Bird ML, Talevski J. Effect of pilates exercise for improving balance in older adults: A systematic review with meta-analysis. Arch Phys Med Rehabil. 2015; 96(4):715-23. [DOI:10.1016/j.apmr.2014.11.021] [PMID]
- Alhasan H, Hood V, Mainwaring F. The effect of visual biofeedback on balance in elderly population: A systematic review. Clin Interv Aging. 2017; 12:487-97. [DOI:10.2147/CIA.S127023] [PMID] [PMCID]
- Neri SG, Cardoso JR, Cruz L, Lima RM, de Oliveira RJ, Iversen MD, et al. Do virtual reality games improve mobility skills and balance measurements in community-dwelling older adults? Systematic review and meta-analysis. Clin Rehabil. 2017; 31(10):1292-304. [DOI:10.1177/0269215517694677] [PMID]
- Li Y, Gao Y, Hu S, Chen H, Zhang M, Yang Y, et al. Effects of multicomponent exercise on the muscle strength, muscle endurance and balance of frail older adults: A meta-analysis of randomised controlled trials. J Clin Nurs. 2023; 32(9-10):1795-805. [DOI:10.1111/jocn.16196] [PMID]
- Cadore EL, Rodríguez-Mañas L, Sinclair A, Izquierdo M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuvenation Res. 2013; 16(2):105-14. [DOI:10.1089/rej.2012.1397] [PMID] [PMCID]
- Aradmehr M, Sagheeslami A, Ilbeigi S. [The effect of balance training and pilates on static and functional balance of elderly men (Persian)]. Feyz Med Sci J. 2015; 18(6):571-7. [Link]
- Lesinski M, Hortobágyi T, Muehlbauer T, Gollhofer A, Granacher U. Effects of balance training on balance performance in healthy older adults: A systematic review and meta-analysis. Sports Med. 2015; 45(12):1721-38. [DOI:10.1007/s40279-014-0284-5] [PMID] [PMCID]
- Kalapotharakos VI, Diamantopoulos K, Tokmakidis SP. Effects of resistance training and detraining on muscle strength and functional performance of older adults aged 80 to 88 years. Aging Clin Exp Res. 2010; 22(2):134-40. [DOI:10.1007/BF03324786] [PMID]
- Pedersen MT, Vorup J, Nistrup A, Wikman JM, Alstrøm JM, et al. Effect of team sports and resistance training on physical function, quality of life, and motivation in older adults. Scand J Med Sci Sports. 2017; 27(8):852-64. [DOI:10.1111/sms.12823] [PMID]
- Hewett TE, Ford KR, Xu YY, Khoury J, Myer GD. Effectiveness of neuromuscular training based on the neuromuscular risk profile. Am J Sports Med. 2017; 45(9):2142-7. [DOI:10.1177/0363546517700128] [PMID] [PMCID]
- Hosseini SS, Rostamkhany H, Naghiloo Z, Lotfi N. The effects of balance, mental and concurrent training on balance in healthy older males. J Res Rehabil Sci. 2010; 6(2):159-67. [DOI:10.22122/jrrs.v6i2.133]
- Aglamiş B, Toraman NF, Yaman H. Change of quality of life due to exercise training in knee osteoarthritis: SF-36 and WOMAC. J Back Musculoskelet Rehabil. 2009; 22(1):43-5, 47-8, 46. [DOI:10.3233/BMR-2009-0219] [PMID]
- Trzepacz PT, Hochstetler H, Wang S, Walker B, Saykin AJ; Alzheimer’s Disease Neuroimaging Initiative. Relationship between the montreal cognitive assessment and mini-mental state examination for assessment of mild cognitive impairment in older adults. BMC Geriatr. 2015; 15:107. [DOI:10.1186/s12877-015-0103-3] [PMID] [PMCID]
- Negahban H, Bavarsad Cheshmeh Ali M, Nassadj G. Effect of hearing aids on static balance function in elderly with hearing loss. Gait Posture. 2017; 58:126-9. [DOI:10.1016/j.gaitpost.2017.07.112] [PMID]
- Zarei H, Norasteh AA. The effect of 8 weeks proprioception training without visual input on single-limb standing balance time in deaf students: A randomized controlled trial. J Bodyw Mov Ther. 2020; 24(2):63-8. [DOI:10.1016/j.jbmt.2020.05.003]
- Martínez-Amat A, Hita-Contreras F, Lomas-Vega R, Caballero-Martínez I, Alvarez PJ, Martínez-López E. Effects of 12-week proprioception training program on postural stability, gait, and balance in older adults: A controlled clinical trial. J Strength Cond Res. 2013; 27(8):2180-8. [DOI:10.1519/JSC.0b013e31827da35f] [PMID]
- Clark VM, Burden AM. A 4-week wobble board exercise programme improved muscle onset latency and perceived stability in individuals with a functionally unstable ankle. Phys Ther Sport. 2005; 6(4):181-7. [DOI:10.1016/j.ptsp.2005.08.003]
- Carmeli E, Zinger-Vaknin T, Morad M, Merrick J. Can physical training have an effect on well-being in adults with mild intellectual disability? Mech Aging Dev. 2005; 126(2):299-304. [DOI:10.1016/j.mad.2004.08.021] [PMID]
- Alfieri FM, Riberto M, Gatz LS, Ribeiro CP, Lopes JA, Battistella LR. Comparison of multisensory and strength training for postural control in the elderly. Clin Interv Aging. 2012; 7:119-25. [DOI:10.2147/CIA.S27747] [PMID] [PMCID]
- Aberson CL. Statistical power analysis. In: Scott RA, Kosslyn SM, et al. Emerging trends in the social and behavioral sciences: An interdisciplinary, searchable, and linkable resource. New Jersey: Wiley; 2015. [DOI:10.1002/9781118900772.etrds0319]
- Casonatto J, Yamacita CM. Pilates exercise and postural balance in older adults: A systematic review and meta-analysis of randomized controlled trials. Complement Ther Med. 2020; 48:102232. [DOI:10.1016/j.ctim.2019.102232] [PMID]
- Shahrbanian S, Hashemi A, Hemayattalab R. The comparison of the effects of physical activity and neurofeedback training on postural stability and risk of fall in elderly women: A single-blind randomized controlled trial. Physiother Theory Pract. 2021; 37(2):271-8. [DOI:10.1080/09593985.2019.1630877] [PMID]
- Karakaya MG, Rutbİl H, Akpinar E, Yildirim A, Karakaya İÇ. Effect of ankle proprioceptive training on static body balance. J Phys Ther Sci. 2015; 27(10):3299-302. [DOI:10.1589/jpts.27.3299] [PMID] [PMCID]
- Alahmari KA, Kakaraparthi VN, Reddy RS, Silvian P, Tedla JS, Rengaramanujam K, et al. Combined effects of strengthening and proprioceptive training on stability, balance, and proprioception among subjects with chronic ankle instability in different age groups: Evaluation of clinical outcome measures. Indian J Orthop. 2020; 55(Suppl 1):199-208. [DOI:10.1007/s43465-020-00192-6] [PMID] [PMCID]
- Lizardo FB, Ronzani GM, Sousa LR, Silva DCdO, Santos LAd, Lopes PR, et al. Proprioceptive exercise with bosu maximizes electromyographic activity of the ankle muscles. Biosci J. 2017; 2017:754-62. [DOI:10.14393/BJ-v33n3-32840]
- Wang Q, Li L, Mao M, Sun W, Zhang C, Mao D, et al. The relationships of postural stability with muscle strength and proprioception are different among older adults over and under 75 years of age. J Exerc Sci Fit. 2022; 20(4):328-34. [DOI:10.1016/j.jesf.2022.07.004] [PMID] [PMCID]
- Pizzigalli L, Filippini A, Ahmaidi S, Jullien H, Rainoldi A. Prevention of falling risk in elderly people: The relevance of muscular strength and symmetry of lower limbs in postural stability. J Strength Cond Res. 2011; 25(2):567-74. [DOI:10.1519/JSC.0b013e3181d32213] [PMID]
- Walsh GS, Low DC, Arkesteijn M. The relationship between postural control and muscle quality in older adults. J Mot Behav. 2022; 54(3):363-71. [DOI:10.1080/00222895.2021.1977602] [PMID]
- Kachouri H, Borji R, Baccouch R, Laatar R, Rebai H, Sahli S. The effect of a combined strength and proprioceptive training on muscle strength and postural balance in boys with intellectual disability: An exploratory study. Res Dev Disabil. 2016; 53-54:367-76. [DOI:10.1016/j.ridd.2016.03.003] [PMID]
- Gidu DV, Badau D, Stoica M, Aron A, Focan G, Monea D, et al. The effects of proprioceptive training on balance, strength, agility and dribbling in adolescent male soccer players. Int J Environ Res Public Health. 2022; 19(4):2028. [DOI:10.3390/ijerph19042028] [PMID] [PMCID]
Type of Study: Research |
Subject:
General
Received: 2024/09/11 | Accepted: 2025/02/27 | Published: 2025/04/1
Received: 2024/09/11 | Accepted: 2025/02/27 | Published: 2025/04/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
