Sat, Dec 27, 2025
Volume 10, Issue 3 (Summer 2024)
Caspian J Neurol Sci 2024, 10(3): 198-209 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sisakhti M, Batouli S A H, Delazar E, Farrahi H. The Digit Span Test: Normative Data for the Iranian Normal Population. Caspian J Neurol Sci 2024; 10 (3) :198-209
URL: http://cjns.gums.ac.ir/article-1-700-en.html
URL: http://cjns.gums.ac.ir/article-1-700-en.html



1- Department of Cognitive Psychology, Institute for Cognitive Sciences Studies, Tehran, Iran.
2- Department of Neuroscience and Addiction Studies, School of Advanced Technologies in Medicine, Tehran University of Medical Sciences, Tehran, Iran.
3- Department of Psychiatry, Faculty of Medicine, Kavosh Cognitive Behavior Sciences and Addiction Research Center, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Psychiatry, Faculty of Medicine, Kavosh Cognitive Behavior Sciences and Addiction Research Center, Guilan University of Medical Sciences, Rasht, Iran. ,h.farrahi14@gmail.com
2- Department of Neuroscience and Addiction Studies, School of Advanced Technologies in Medicine, Tehran University of Medical Sciences, Tehran, Iran.
3- Department of Psychiatry, Faculty of Medicine, Kavosh Cognitive Behavior Sciences and Addiction Research Center, Guilan University of Medical Sciences, Rasht, Iran.
4- Department of Psychiatry, Faculty of Medicine, Kavosh Cognitive Behavior Sciences and Addiction Research Center, Guilan University of Medical Sciences, Rasht, Iran. ,
Full-Text [PDF 1675 kb]
(2642 Downloads)
| Abstract (HTML) (1406 Views)
Full-Text: (2012 Views)
Introduction
As an interdisciplinary science, neuropsychology aims to identify the relationship between the brain and behavior, specifically the effects of brain functioning on mental and behavioral processes [1]. It is one of the most important scientific fields with advanced methods that are expected to help measure and make decisions about the diagnosis, rehabilitation and treatment planning, forensic determination, educational planning, the baseline of function for subsequent testing, capacity for independent living, pre and post-medical intervention, and localization of a lesion [2]. Although one of the important goals of neuropsychology at the beginning was to help localize brain lesions, with the advent and development of imaging technologies, the primary goals of neuropsychology have expanded and leaned to understand the behavioral and cognitive effects of brain function and dysfunction [3]. Neuropsychology often uses assessment tools to achieve its goals [4]. These tools, often self-administered or clinician-administered, are designed to give a specific or comprehensive picture of people’s behavioral and cognitive abilities and capacities [5]. The findings of such evaluations have significant clinical or prognostic value, especially for people with neurocognitive problems and can be effective in improving treatment or prevention [6].
Typically, the domains measured by neuropsychological tools include attention, language, visuospatial, memory and executive functions [7, 8]. Although it is desirable that neuropsychological tools precisely measure a specific ability or domain, due to the complexity of these abilities and the relatively extensive involvement of brain areas in performing various neurocognitive functions, including higher brain functions, neuropsychological tools often measure multiple skills at the same time [7, 8]. The digit span test (DST) is one of the most widely used neuropsychological tools that is usually used to measure attention, working memory, and immediate recall [9, 10]. In the last few decades, an extensive literature has been produced about its psychometric properties and clinical and research applications [11]. Based on the survey conducted by the National Academy of Neuropsychology and the International Neuropsychological Society (INS), DST was the most frequently used measure of attention, concentration and working memory [2]. The test consists of two parts or modalities: Forward and backward. In the forward digit span test (fDST), different sequences of digits are read to the subjects, and they are asked to repeat them. In the backward digit span test (bDST), the subjects are asked to repeat the digits in reverse (from the last to the first). The cognitive functions measured in the forward and backward subtests differ. While fDST primarily measures attention-related abilities, bDST assesses working memory [12].
DST is one of the subtests of two well-known scales of intelligence and memory: The Wechsler adult intelligence scale (WAIS) and the Wechsler memory scale (WMS) [13]. Also, it has been widely used both independently and as part of various neuropsychological test batteries. The DST has been used to assess attention and working memory in a wide range of diseases, such as Alzheimer [14], epilepsy [15], mild cognitive impairment [16], and schizophrenia [17]. Also, the cognitive performance of normal people, such as drivers [18], veterans [19], and pilots [20], are measured using DST. In addition, DST has been used in different age groups, including children [21], adults [22] and older people [23]. Besides the independent application of DST, it is included as one of the subtests of several neuropsychological test batteries, such as the neuropsychological test battery from the uniform data set of the alzheimer disease centers [24], the Toronto cognitive assessment for detecting amnestic mild cognitive impairment [25] and the Chinese brief cognitive test [26].
Although some tests, including digit-based measures, are less dependent on culture than others, gathering normative data based on demographic variables is necessary to understand better and measure the possible deficit [7]. According to the search in scientific databases, there have been many studies to collect normative data on attention and working memory performance in the DST in different languages such as English [27], Filipino [28], Spanish [29], Dutch [30], Arabic [31] and Korean [32]. Although the results regarding the effect of gender on performance in DST are heterogeneous, many normative data studies indicate that increasing age and education have decreasing and increasing impacts on performance in the DST, respectively [28-32].
Among the common problems faced by neuropsychologists in evaluating the psychological and behavioral changes of the brain and related disorders in many countries are 1) Insufficient normative data for neuropsychological tools in their countries, 2) Inapplicability of language-based neuropsychological tools for illiterate patients, 3) High cost and 4) Lack of cultural adaptations [33]. Neuropsychological assessment in Iran also faces such problems, and many neurocognitive assessment tools lack Iranian normative data, so the examiner may have to refer to normative data collected in developed countries (mainly North America) to perform neuropsychological assessment of people with typical or atypical brain functioning. To the best of our knowledge, despite the high importance and widespread use of the DST, its normative data has not yet been collected separately and independently in Iran. This test has the advantage of being independent of literacy and inexpensive to administer. Also, it does not require cultural adaptation due to its reliance on a few digits that are presented audibly. Considering the increasing use of neuropsychological evaluations and the need to access regional normative data, the present study aimed to 1) Collect the normative data appropriate to the Iranian population, 2) Cover a longer age range (ages 20 to 70) and 3) Have both genders equally present in the study sample. In addition to the above objectives, we sought to find whether, like some normative data in the populations of other countries [28-32], demographic variables of age, gender, and education affect the neurocognitive functions of attention and working memory assessed by the DST in the Iranian population.
Materials and Methods
Study data
The present study was conducted in 2017-2018 as part of the Iranian brain imaging database (IBID) project to collect normative measures of the structural and functional properties of the brains of Iranian normal people for future investigation and interventional purposes [34-36]. To complete these normative data, a series of well-known and widely-used neuropsychological tests were implemented on the Iranian normal population. The tests were performed in the same order and on one day. As a result, a considerable neural and cognitive database was gathered for further analysis. DST was one of the cognitive tests that was performed to evaluate working memory and attention. The research sample consisted of 300 normal people aged 20 to 70. Each decade consisted of 60 participants, and the gender proportion was equal. In addition, according to some previous studies on neuropsychological measures [37, 38], two levels of diploma/sub-diploma and higher diploma were used to investigate the effect of education level on the DST scores. Five decades of age (20 to 70 years old), gender, and years of education were the independent variables, and scores obtained in DST (defined as two scores of the longest digit sequence and total digit span obtained in two subtests of forward DST and backward DST) were the dependent variable.
Study procedure
The recruitment of participants in the research was based on advertisements in local media and social networks (for more complementary information, see Batouli et al. [34], Sisakhti et al. [35, 36] and Batouli and Sisakhti [39]). To exclude individuals with cognitive, medical, and mental health problems, all participants were interviewed twice by a general practitioner and a trained cognitive psychologist. In addition, after entering participants in the study and gathering their data, if the obtained scores in cognitive and mental health tests were extreme outliers (≥3.3≥ standard deviations), they were excluded from the sample [34-36]. The inclusion criteria were speaking fluently in Farsi, having the ability to read and write, and being between 20 and 70 years old. The exclusion criteria consisted of having a history of consuming illicit drugs, systemic, psychiatric, and neurological illness, the current use of any medication affecting neurocognitive performance and visual and auditory defects affecting performance in tests. Due to the duration of the project and the necessity of a long presence of the participants, a small gift was given to them. Participants entered the study voluntarily and signed a written consent before implementing the study measures. The present study was approved by the Ethics Committee of the National Institute for Medical Research Development (NIMAD) (for more information on the IBID project, inclusion and exclusion criteria and methods, see Batouli et al. [34]).
Study measure
The DST measures working memory and attention, which was first developed as one of the subscales of WAIS and WMS [13]. In addition, it is implemented as an independent test or one of the subtests of several neuropsychological test batteries in clinical and research settings [24-26]. The subject must remember and repeat the digits read by the examiner in the correct order. Correct answers require a two-step process. First, the digits must be received carefully, which requires attention and decoding. Second, the subject must remember the digits correctly, consider their order and sequence, and pronounce them. The DST consists of two modalities: Forward (fDST) and backward (bDST). In the fDST, the subject is asked to repeat the numbers read by the examiner in the same order, while in the bDST, the subject must say the digits in reverse order (from end to beginning). In the forward subtest, the number of digits in each string increases from 3 to 9 and in the backward subtest from 2 to 8. The testing is stopped when the subject cannot answer correctly in two consecutive trials [40]. The fDST is an easier task for subjects than the bDST. The subject has to keep the information in memory longer than the fDST and change their order before retelling it. Better performance in the bDST may indicate a person’s ability to be flexible, focused and resilient under stress. A higher score on backward digits may also be related to the ability to form, hold and scan visual mental images from auditory stimuli [13]. This subtest is highly vulnerable to anxiety. A huge difference between direct and reverse numbers can be a marker of organic brain damage. While the low score of forward digits is more likely to be seen in the left hemisphere lesion, the low score in the case of backward digits is more likely to be observed in the right frontal lesion [13].
Statistical analysis
To analyze the research data, after describing the subjects by descriptive statistics using central (Mean±SD) indicators (Table 1), Pearson's and Spearman's correlation coefficients were used to determine the correlation of age with the DST scores and the correlation of education and gender with the DST scores, respectively (Table 2).
Levene’s test was used to examine the homogeneity of variances (Table 3).
In addition, multivariate analysis of variance (MANOVA) was used to explore the differences between the subjects in terms of age, gender, education, and the interaction of these variables in the DST scores (Tables 4 and 5).
Also, Tukey's post hoc test was used to investigate the difference between each age group and other groups in each score (Table 6).
A P<0.05 was considered statistically significant.
Results
The total number of participants was 300. The sample’s age range was 20–70 years, with 60 participants in each decade of age and an equal proportion of genders in each group. Most participants had a diploma and BS or MS, and the frequency of participants with under-diploma or doctorate education was low.
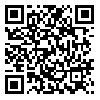
The Mean±SD of the total digit span in the fDST were 8.09 and 1.95 and the longest digit sequences were 5.54 and 1.21, respectively. Also, in bDST, the Mean±SD of the total digit span were 6.09 and 2.03, and the longest digit sequences were 4.6 and 1.26, respectively. Table 1 shows the participants’ Mean±SD and minimum and maximum scores (range of changes) classified by age, gender, and education. As can be seen, in most cases, with increasing age, the total digit span scores and the longest digit sequence of participants in both subtests have decreased. Also, participants with more than 12 years of education had higher scores in both the total digit span and the longest digit sequence.
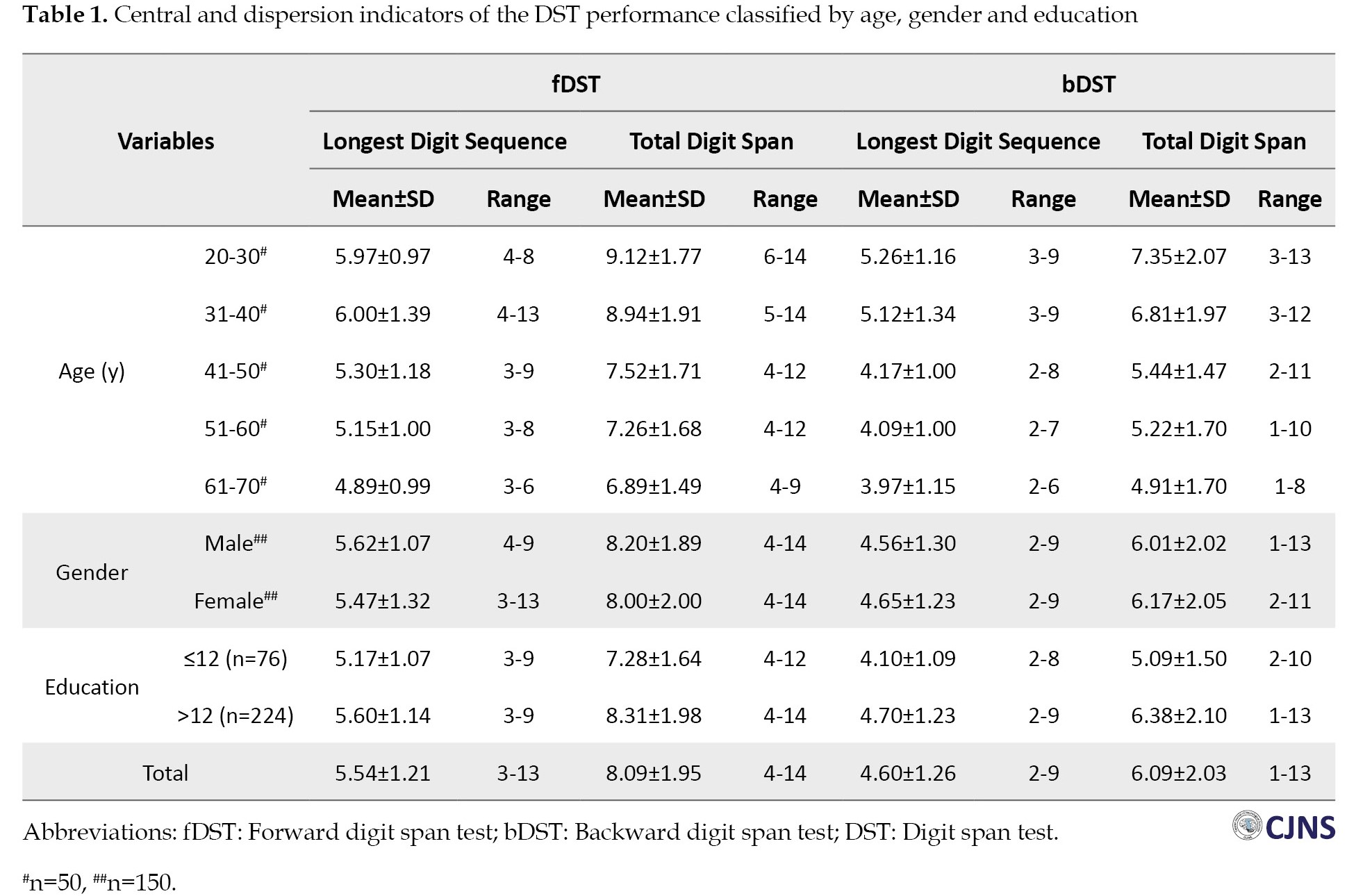
As shown in Table 2, the Pearson correlation coefficient reveals that age has a significant reverse correlation with the total digit span and the longest digit sequence in both subtests (P=0.01). This means that the total digit span and the longest digit sequence of the fDST and the bDST decreased with age. Also, the Spearman correlation coefficient shows that education has a significant direct correlation with the total digit span scores and the longest digit sequence in both tests (P<0.01), which means that the total digit span and the longest digit sequence of the fDST and bDST increase with increasing education. However, based on the Spearman correlation coefficient, no significant correlation was observed between gender and scores (P>0.05).
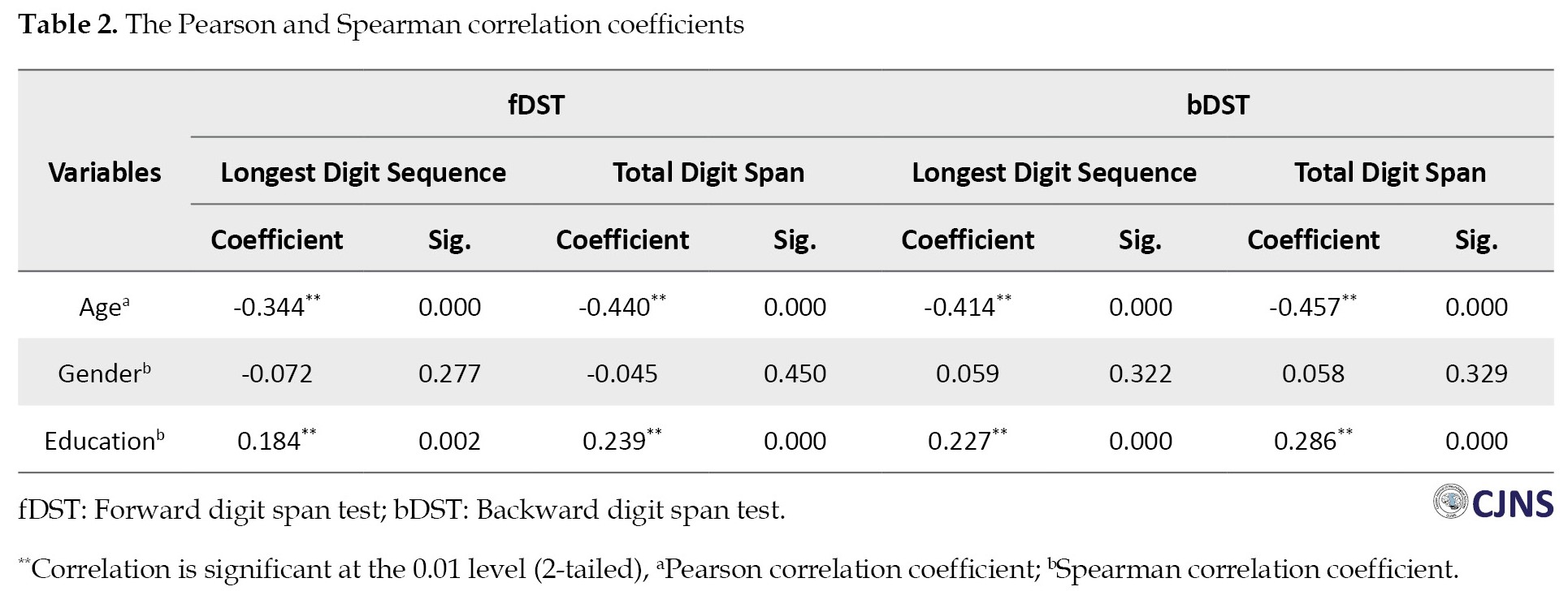
Levene’s test was used to examine the homogeneity of variances. Based on this test, the assumption of homogeneity of variances in the case of the total digit span (P=0.562) and the longest digit sequence (P=0.616) of the fDST, and the total digit span (P=0.264) and the longest digit sequence (P=0.149) of the bDST were confirmed (Table 3).
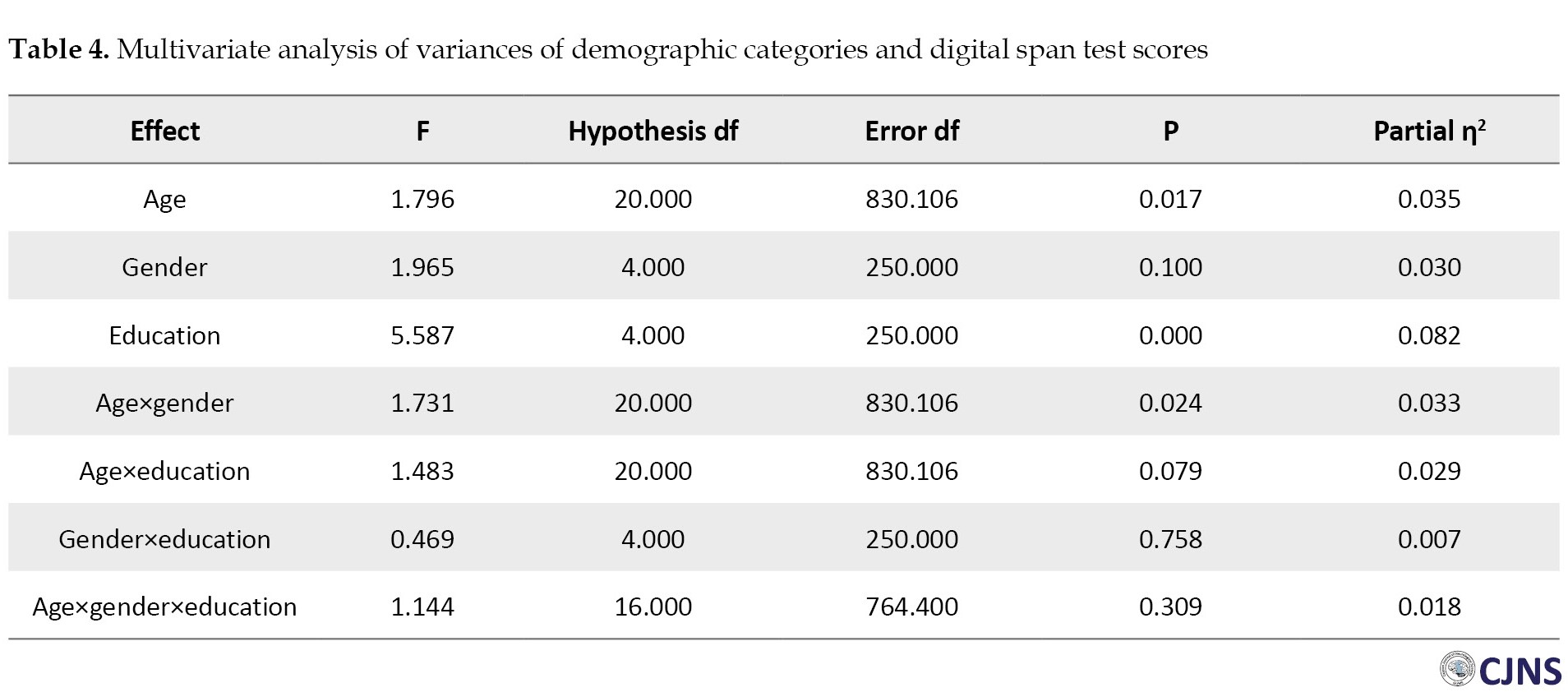
As shown in Table 4, MANOVA displays a significant difference in the DST scores between different age groups (F=1.796, P=0.017) and education levels (F=5.587, P=0.0001). In contrast, this difference does not exist between the two genders (F=1.965, P=0.1). The difference in the DST scores is seen between men and women in different age groups (F=1.731, P=0.024). At the same time, there was no difference among participants with academic education and those with sub-academic education in age groups (F=1.483, P=0.079) and between the two genders (F=0.469, P=0.758). Also, the interaction of age, gender and education did not lead to a significant difference in the DST scores (F=1.144, P=0.309).
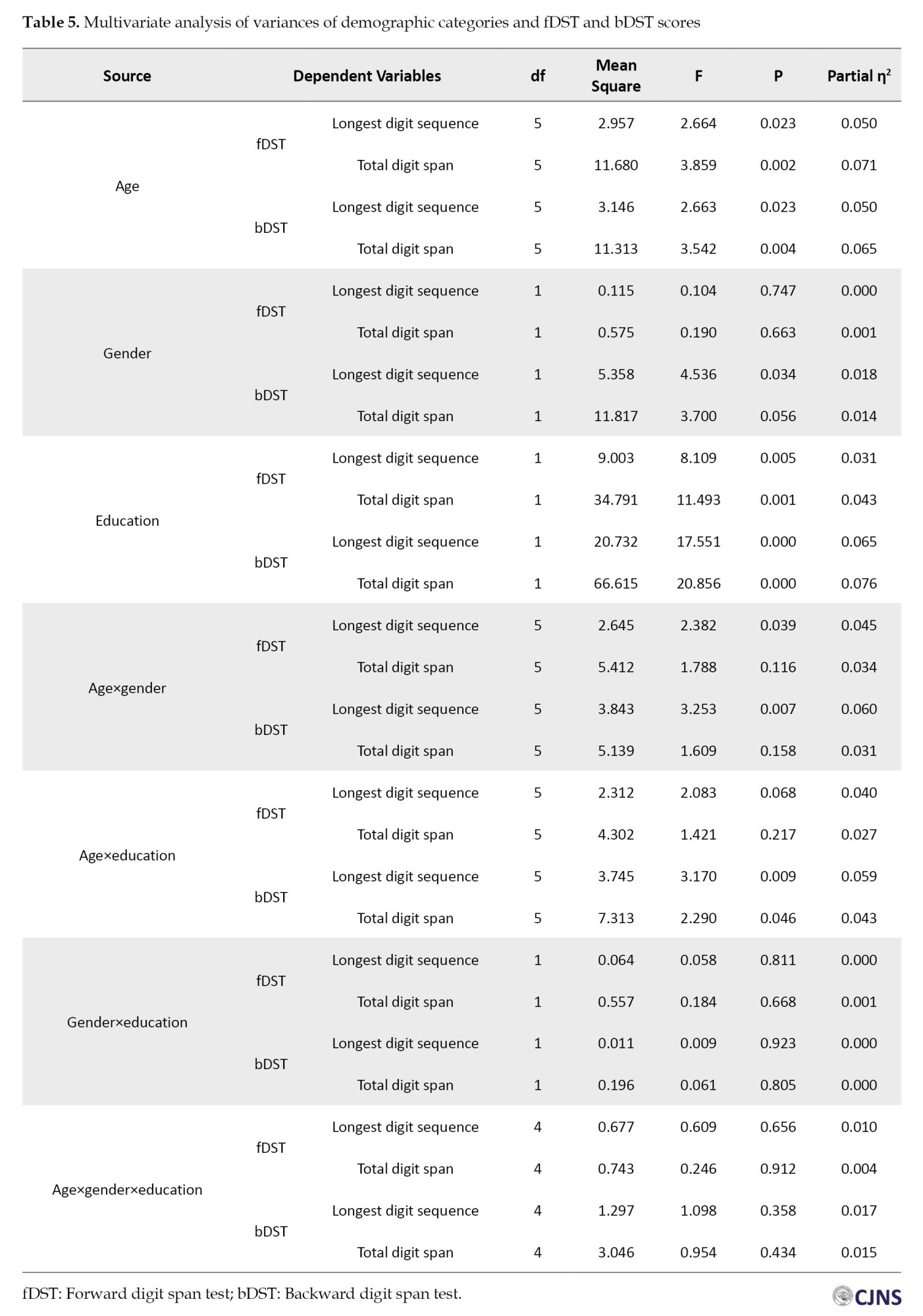
Table 5 shows the differences between participants in different demographic categories in terms of the total digit span and the longest digit sequence of two subtests of the DST. As seen, participants of five age groups have significant differences in all four DST scores (the fDST longest digit sequence: F=2.664, P=0.023; the fDST total digit span: 3.859, P=0.002; the bDST longest digit sequence: F=2.663, P =0.023 and the bDST total digit span: F=3.354, P=0.004). Women and men have a significant difference in the bDST longest sequence (F=4.536, P=0.034), which according to Table 1, Mean±SD of men (4.65±1.23) have a higher score than Mean±SD of women (4.56±1.30). However, there was no difference in the fDST total digit span (F=0.190, P=0.663), the fDST longest digit sequence (F=0.104, P=0.747) and the bDST total digit span (F=3.7, P=0.056) among women and men. Participants with academic education differed from those with sub-academic education in terms of all scores (the fDST longest digit sequence: F=8.109, P=0.005; the fDST total digit span: F=11.493, P=0.001; the bDST longest digit sequence: F=17.551, P=0.001 and the bDST total digit span: F=20.856, P=0.000). According to Table 1, participants with an academic education (the fDST Mean±SD longest digit sequence: 5.60±1.14; the fDST Mean±SD total digit span: 8.31±1.98; the bDST Mean±SD longest digit sequence: 4.70±1.23; and the bDST Mean±SD total digit span: 6.38±2.10) in all scores were higher than those with sub-academic education (the fDST Mean±SD longest digit sequence: 5.17±1.07; the fDST Mean±SD total digit span: 7.28±1.64; the bDST Mean±SD longest digit sequence: 4.10±1.09; and the bDST Mean±SD total digit span: 5.09±1.50). Men and women in different age groups also differed from each other in terms of the fDST longest sequence (F=2.382, P=0.039) and the bDST longest sequence (F=3.253, P=0.007). Also, the participants with academic education were different from those with sub-academic education in different age groups in terms of the bDST total digit span (F=3.17, P=0.009) and the bDST longest digit sequence (F=2.29, P=0.046).
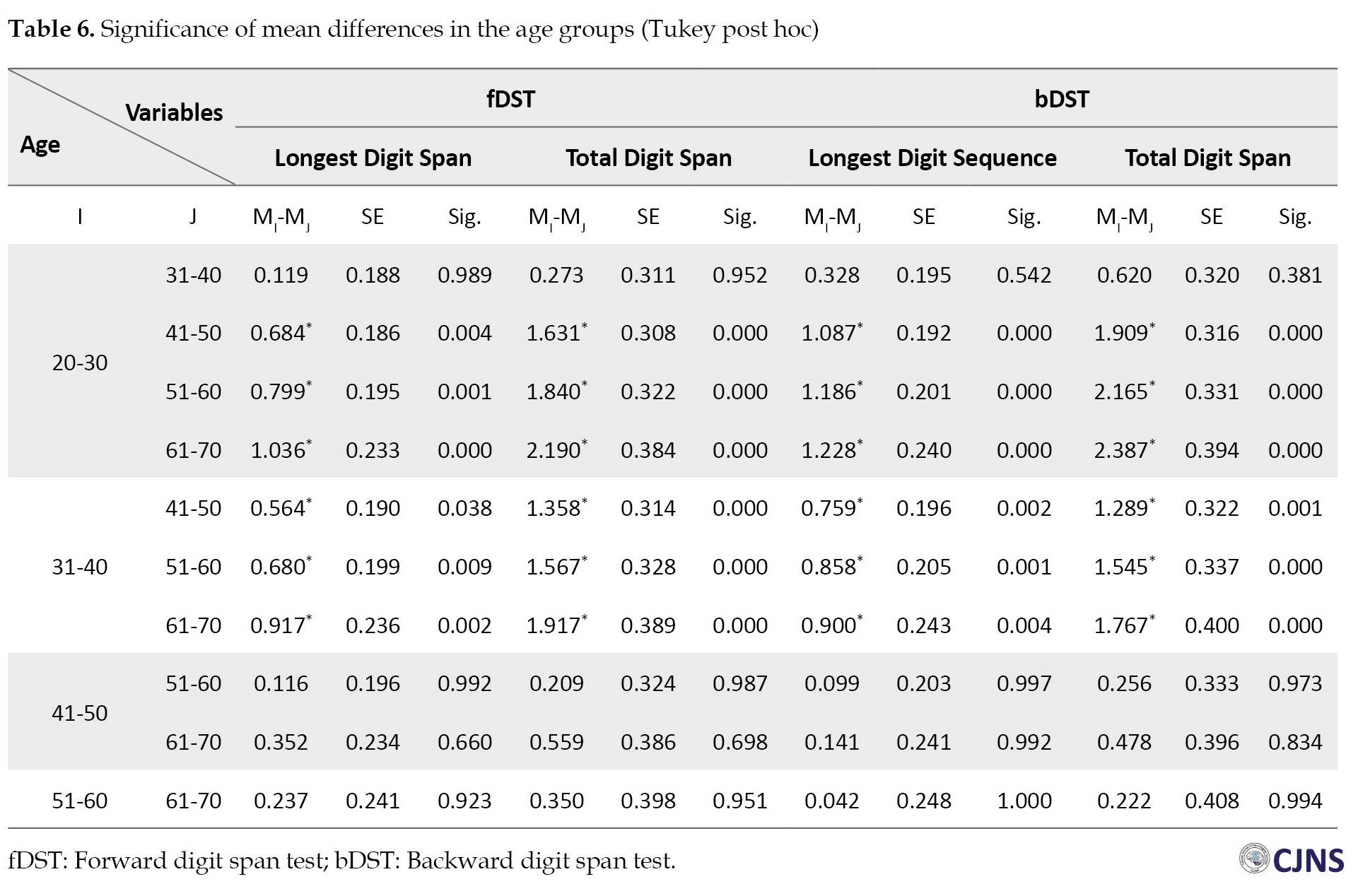
Table 6 presents the results of the Tukey post hoc test to examine the differences in the DST scores in the age groups of participants. In both DST subtests, participants under 40 had significantly higher total digit span and longest digit sequence than older participants (P<0.05). However, participants aged 40 to 70 did not differ in this respect (P>0.05).
Discussion
In this study, we aimed to collect Iranian normative data on one of the most well-known and widely-used tests of working memory and attentional capacity. We also examined whether the three demographic variables of age, education, and gender affect the performance of normal people in the forward and backward subtests of DST. Our findings showed that age had a significant negative correlation with both fDST and bDST, which means that the performance in DST decreased with age. Unlike age, education had a significant positive correlation with both subtests, which means that the performance in DST increases with increasing education level. However, there was no significant correlation between gender and DST scores. In addition, MANOVA showed a significant difference in DST scores between different age groups and education levels, with no difference between the two genders.
Our study demonstrated that the performance in DST as a measure of memory span and attentional capacity declines with age. The literature shows the significant effects of some demographic variables like age on different domains of cognitive functioning [41]. In particular, it has been demonstrated that aging is associated with performance decline in some cognitive capacities and functions [24, 41]. A study of 723 normal Chinese adult participants found that younger adults performed better on DST [41]. In another study of 164 individuals without cognitive complaints, age showed an inverse correlation with the scores obtained in DST, while education and gender did not have a significant relationship [31]. A decremental effect of age on DST performance at older ages has also been reported. A study of 3268 cognitively normal older adults found that increasing age is related to decreasing DST scores [24]. Also, in a study of 784 people aged 60-90 without serious neurological, medical and psychiatric complaints, DST performance decreased with older age [32].
Despite many studies favoring the decremental effect of aging on DST performance, some studies have not shown such an effect. In a sample of Spanish-speaking normal people over 55, age was not correlated to the DST performance [29]. Another study investigating the effect of increasing age on the cognitive functioning of 658 adults aged 60-84 found that increasing age did not affect DST performance [42]. In addition, in a study of 332 cognitively normal Spanish adults, no decremental effect of age was found [43]. This finding was repeated in two other studies on Hispanic adults aged 75-19 years [44] and 75-16 years [45]. In explaining the findings related to the lack of association between age and DST performance, some researchers have pointed out the simplicity of responding to DST stimuli and the difference in the research samples. It has been suggested that tests like DST are simpler than more complex tests like the symbol digit modalities test, and the effect of age is less visible [46].
According to our other finding, higher levels of education are associated with increased participants’ performance in DST. This finding is consistent with the results of many studies [43, 44, 41, 32, 24]. The relationship between education and DST performance is strong in many studies, and it is even observed without an association between age and DST scores. A study of 2574 Spanish-speaking participants found that the level of education is a stronger predictor of performance than age in both fDST and bDST [38]. In Spanish multicenter normative studies (NEURONORMA project) on 354 cognitively intact participants aged 50 to 90, although both age and education were related to performance on DST, the effect of education was greater than age [46]. In a sample of Spanish-speaking normal people over 55, age and gender were unrelated to fDST and bDST, and education was significantly associated with both modalities [22]. The effect of education on DST performance is so strong that even in people over 100 years of age (centenarians), this significant association has been observed [30].
In general, although some studies have documented the cognitive similarities of the two genders more than their differences [47], gender differences in various neuropsychological domains have been systematically reported in the literature [48]. However, our findings showed no association between DST performance and gender. The effect of gender on DST performance has been controversial in the literature [32]. Many studies have not reported such an effect [32, 43, 24]. A study of 723 normal Chinese adult participants found no significant difference between the two genders in DST performance [41]. Also, in a sample of Spanish-speaking normal people over 55 years old, gender was unrelated to fDST and bDST [22]. In another study, researchers examined the question of whether gender differences in working memory are related to the nature of the stimuli (verbal vs visuospatial). These researchers used forward and backward modalities of two working memory tests (Corsi block-tapping test with visuospatial stimuli and DST with verbal stimuli) to investigate this question. Their findings showed that both genders had no significant difference in fDST and bDST, while in the Corsi test, a significant difference was observed between them [49]. Men’s superiority in visuospatial processing over women has been proposed to explain such findings. This superiority can have an evolutionary origin [50]. More findings in support of this finding are obtained from studies that show that men have a significant advantage over women in tasks that require mental rotation [51].
A final point is worth noting here. One obvious benefit of providing normative data is that it can be used to interpret individual scores. Since most neuropsychological tests are standardized on normal populations, reporting the Mean±SD of the normative sample often allows a comparison between individual and normative scores. According to the commonly recommended rule in interpreting neuropsychological tests, 1.5 standard deviations below the normative mean indicate that a person’s performance was worse than approximately 93.3% of the normative sample. According to this rule, -1.5, -1.7, -2.0, -2.5 and -3.0 standard deviations below the normative mean will indicate mild, mild to moderate, moderate, severe and most severe levels of impairment, respectively [52].
Conclusion
In sum, our study, in addition to providing normative data for the well-known and widely-used measure of attention and working memory, the DST, showed that the two demographic variables of age and education significantly correlate with the fDST and bDST modalities. In contrast, gender did not show such an association. Considering the rapid aging of the population in Iran and the need for neuropsychological tools for diagnosis, treatment, prevention, and rehabilitation, our results help clinicians interpret the results of neuropsychological tests more accurately and reduce the possibility of false diagnoses of cognitive impairment. The findings of our study emphasize the importance of clinicians’ access to appropriate normative data for the Iranian population.
Limitations and future research
There are several limitations in our study. First, the education level of most participants in the study was higher than the diploma, and there were very few participants with an education lower than a diploma. The presence of equal or relatively equal proportions of participants with different levels of education in future studies can help to generalize the obtained results. Second, the sample used in our study was relatively small. This sample size may not be enough to generalize the results to the healthy Iranian population. It is recommended that a larger sample be used in future studies to collect normative data on the Iranian population. Third, the research sample was analyzed based on the three variables of age, sex, and education without differentiating them based on ethnicity, race, socioeconomic status and cultural factors. Considering the variables of ethnicity, race, socioeconomic status, and cultural factors may be important to collect normative data. Classifying the research sample based on the above variables in future studies can increase our understanding of the effect of different demographic variables on cognitive performance. It can provide more accurate normative data for clinical and research settings.
Ethical Considerations
Compliance with ethical guidelines
All study procedures were in compliance with the ethical guidelines of the 2013 Declaration of Helsinki. The present study was approved by the Ethics Committee of the National Institute for Medical Research Development (NIMAD) (Code: IR NIMAD REC.1396.319). Participation in the study was voluntary and written consent was obtained from all participants.
Funding
This study was financially supported by the Iranian National Institute for Medical Research Development (NIMAD) (Grant No.: 962550).
Authors contributions
Conceptualization, validation and methodology: Minoo Sisakhti and Seyed Amir Hossein Batouli; Statistical analysis: Hassan Farrahi and Elaheh Delazar; Supervision, investigation and data curation: Minoo Sisakhti and Seyed Amir Hossein Batouli; Writing the original draft: Hassan Farrahi and Elaheh Delazar; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank all the participants in the various stages of the present study, from interviewing and testing to structural and functional imaging.
References
As an interdisciplinary science, neuropsychology aims to identify the relationship between the brain and behavior, specifically the effects of brain functioning on mental and behavioral processes [1]. It is one of the most important scientific fields with advanced methods that are expected to help measure and make decisions about the diagnosis, rehabilitation and treatment planning, forensic determination, educational planning, the baseline of function for subsequent testing, capacity for independent living, pre and post-medical intervention, and localization of a lesion [2]. Although one of the important goals of neuropsychology at the beginning was to help localize brain lesions, with the advent and development of imaging technologies, the primary goals of neuropsychology have expanded and leaned to understand the behavioral and cognitive effects of brain function and dysfunction [3]. Neuropsychology often uses assessment tools to achieve its goals [4]. These tools, often self-administered or clinician-administered, are designed to give a specific or comprehensive picture of people’s behavioral and cognitive abilities and capacities [5]. The findings of such evaluations have significant clinical or prognostic value, especially for people with neurocognitive problems and can be effective in improving treatment or prevention [6].
Typically, the domains measured by neuropsychological tools include attention, language, visuospatial, memory and executive functions [7, 8]. Although it is desirable that neuropsychological tools precisely measure a specific ability or domain, due to the complexity of these abilities and the relatively extensive involvement of brain areas in performing various neurocognitive functions, including higher brain functions, neuropsychological tools often measure multiple skills at the same time [7, 8]. The digit span test (DST) is one of the most widely used neuropsychological tools that is usually used to measure attention, working memory, and immediate recall [9, 10]. In the last few decades, an extensive literature has been produced about its psychometric properties and clinical and research applications [11]. Based on the survey conducted by the National Academy of Neuropsychology and the International Neuropsychological Society (INS), DST was the most frequently used measure of attention, concentration and working memory [2]. The test consists of two parts or modalities: Forward and backward. In the forward digit span test (fDST), different sequences of digits are read to the subjects, and they are asked to repeat them. In the backward digit span test (bDST), the subjects are asked to repeat the digits in reverse (from the last to the first). The cognitive functions measured in the forward and backward subtests differ. While fDST primarily measures attention-related abilities, bDST assesses working memory [12].
DST is one of the subtests of two well-known scales of intelligence and memory: The Wechsler adult intelligence scale (WAIS) and the Wechsler memory scale (WMS) [13]. Also, it has been widely used both independently and as part of various neuropsychological test batteries. The DST has been used to assess attention and working memory in a wide range of diseases, such as Alzheimer [14], epilepsy [15], mild cognitive impairment [16], and schizophrenia [17]. Also, the cognitive performance of normal people, such as drivers [18], veterans [19], and pilots [20], are measured using DST. In addition, DST has been used in different age groups, including children [21], adults [22] and older people [23]. Besides the independent application of DST, it is included as one of the subtests of several neuropsychological test batteries, such as the neuropsychological test battery from the uniform data set of the alzheimer disease centers [24], the Toronto cognitive assessment for detecting amnestic mild cognitive impairment [25] and the Chinese brief cognitive test [26].
Although some tests, including digit-based measures, are less dependent on culture than others, gathering normative data based on demographic variables is necessary to understand better and measure the possible deficit [7]. According to the search in scientific databases, there have been many studies to collect normative data on attention and working memory performance in the DST in different languages such as English [27], Filipino [28], Spanish [29], Dutch [30], Arabic [31] and Korean [32]. Although the results regarding the effect of gender on performance in DST are heterogeneous, many normative data studies indicate that increasing age and education have decreasing and increasing impacts on performance in the DST, respectively [28-32].
Among the common problems faced by neuropsychologists in evaluating the psychological and behavioral changes of the brain and related disorders in many countries are 1) Insufficient normative data for neuropsychological tools in their countries, 2) Inapplicability of language-based neuropsychological tools for illiterate patients, 3) High cost and 4) Lack of cultural adaptations [33]. Neuropsychological assessment in Iran also faces such problems, and many neurocognitive assessment tools lack Iranian normative data, so the examiner may have to refer to normative data collected in developed countries (mainly North America) to perform neuropsychological assessment of people with typical or atypical brain functioning. To the best of our knowledge, despite the high importance and widespread use of the DST, its normative data has not yet been collected separately and independently in Iran. This test has the advantage of being independent of literacy and inexpensive to administer. Also, it does not require cultural adaptation due to its reliance on a few digits that are presented audibly. Considering the increasing use of neuropsychological evaluations and the need to access regional normative data, the present study aimed to 1) Collect the normative data appropriate to the Iranian population, 2) Cover a longer age range (ages 20 to 70) and 3) Have both genders equally present in the study sample. In addition to the above objectives, we sought to find whether, like some normative data in the populations of other countries [28-32], demographic variables of age, gender, and education affect the neurocognitive functions of attention and working memory assessed by the DST in the Iranian population.
Materials and Methods
Study data
The present study was conducted in 2017-2018 as part of the Iranian brain imaging database (IBID) project to collect normative measures of the structural and functional properties of the brains of Iranian normal people for future investigation and interventional purposes [34-36]. To complete these normative data, a series of well-known and widely-used neuropsychological tests were implemented on the Iranian normal population. The tests were performed in the same order and on one day. As a result, a considerable neural and cognitive database was gathered for further analysis. DST was one of the cognitive tests that was performed to evaluate working memory and attention. The research sample consisted of 300 normal people aged 20 to 70. Each decade consisted of 60 participants, and the gender proportion was equal. In addition, according to some previous studies on neuropsychological measures [37, 38], two levels of diploma/sub-diploma and higher diploma were used to investigate the effect of education level on the DST scores. Five decades of age (20 to 70 years old), gender, and years of education were the independent variables, and scores obtained in DST (defined as two scores of the longest digit sequence and total digit span obtained in two subtests of forward DST and backward DST) were the dependent variable.
Study procedure
The recruitment of participants in the research was based on advertisements in local media and social networks (for more complementary information, see Batouli et al. [34], Sisakhti et al. [35, 36] and Batouli and Sisakhti [39]). To exclude individuals with cognitive, medical, and mental health problems, all participants were interviewed twice by a general practitioner and a trained cognitive psychologist. In addition, after entering participants in the study and gathering their data, if the obtained scores in cognitive and mental health tests were extreme outliers (≥3.3≥ standard deviations), they were excluded from the sample [34-36]. The inclusion criteria were speaking fluently in Farsi, having the ability to read and write, and being between 20 and 70 years old. The exclusion criteria consisted of having a history of consuming illicit drugs, systemic, psychiatric, and neurological illness, the current use of any medication affecting neurocognitive performance and visual and auditory defects affecting performance in tests. Due to the duration of the project and the necessity of a long presence of the participants, a small gift was given to them. Participants entered the study voluntarily and signed a written consent before implementing the study measures. The present study was approved by the Ethics Committee of the National Institute for Medical Research Development (NIMAD) (for more information on the IBID project, inclusion and exclusion criteria and methods, see Batouli et al. [34]).
Study measure
The DST measures working memory and attention, which was first developed as one of the subscales of WAIS and WMS [13]. In addition, it is implemented as an independent test or one of the subtests of several neuropsychological test batteries in clinical and research settings [24-26]. The subject must remember and repeat the digits read by the examiner in the correct order. Correct answers require a two-step process. First, the digits must be received carefully, which requires attention and decoding. Second, the subject must remember the digits correctly, consider their order and sequence, and pronounce them. The DST consists of two modalities: Forward (fDST) and backward (bDST). In the fDST, the subject is asked to repeat the numbers read by the examiner in the same order, while in the bDST, the subject must say the digits in reverse order (from end to beginning). In the forward subtest, the number of digits in each string increases from 3 to 9 and in the backward subtest from 2 to 8. The testing is stopped when the subject cannot answer correctly in two consecutive trials [40]. The fDST is an easier task for subjects than the bDST. The subject has to keep the information in memory longer than the fDST and change their order before retelling it. Better performance in the bDST may indicate a person’s ability to be flexible, focused and resilient under stress. A higher score on backward digits may also be related to the ability to form, hold and scan visual mental images from auditory stimuli [13]. This subtest is highly vulnerable to anxiety. A huge difference between direct and reverse numbers can be a marker of organic brain damage. While the low score of forward digits is more likely to be seen in the left hemisphere lesion, the low score in the case of backward digits is more likely to be observed in the right frontal lesion [13].
Statistical analysis
To analyze the research data, after describing the subjects by descriptive statistics using central (Mean±SD) indicators (Table 1), Pearson's and Spearman's correlation coefficients were used to determine the correlation of age with the DST scores and the correlation of education and gender with the DST scores, respectively (Table 2).
Levene’s test was used to examine the homogeneity of variances (Table 3).
In addition, multivariate analysis of variance (MANOVA) was used to explore the differences between the subjects in terms of age, gender, education, and the interaction of these variables in the DST scores (Tables 4 and 5).
Also, Tukey's post hoc test was used to investigate the difference between each age group and other groups in each score (Table 6).
A P<0.05 was considered statistically significant.
Results
The total number of participants was 300. The sample’s age range was 20–70 years, with 60 participants in each decade of age and an equal proportion of genders in each group. Most participants had a diploma and BS or MS, and the frequency of participants with under-diploma or doctorate education was low.
The Mean±SD of the total digit span in the fDST were 8.09 and 1.95 and the longest digit sequences were 5.54 and 1.21, respectively. Also, in bDST, the Mean±SD of the total digit span were 6.09 and 2.03, and the longest digit sequences were 4.6 and 1.26, respectively. Table 1 shows the participants’ Mean±SD and minimum and maximum scores (range of changes) classified by age, gender, and education. As can be seen, in most cases, with increasing age, the total digit span scores and the longest digit sequence of participants in both subtests have decreased. Also, participants with more than 12 years of education had higher scores in both the total digit span and the longest digit sequence.
As shown in Table 2, the Pearson correlation coefficient reveals that age has a significant reverse correlation with the total digit span and the longest digit sequence in both subtests (P=0.01). This means that the total digit span and the longest digit sequence of the fDST and the bDST decreased with age. Also, the Spearman correlation coefficient shows that education has a significant direct correlation with the total digit span scores and the longest digit sequence in both tests (P<0.01), which means that the total digit span and the longest digit sequence of the fDST and bDST increase with increasing education. However, based on the Spearman correlation coefficient, no significant correlation was observed between gender and scores (P>0.05).
Levene’s test was used to examine the homogeneity of variances. Based on this test, the assumption of homogeneity of variances in the case of the total digit span (P=0.562) and the longest digit sequence (P=0.616) of the fDST, and the total digit span (P=0.264) and the longest digit sequence (P=0.149) of the bDST were confirmed (Table 3).
As shown in Table 4, MANOVA displays a significant difference in the DST scores between different age groups (F=1.796, P=0.017) and education levels (F=5.587, P=0.0001). In contrast, this difference does not exist between the two genders (F=1.965, P=0.1). The difference in the DST scores is seen between men and women in different age groups (F=1.731, P=0.024). At the same time, there was no difference among participants with academic education and those with sub-academic education in age groups (F=1.483, P=0.079) and between the two genders (F=0.469, P=0.758). Also, the interaction of age, gender and education did not lead to a significant difference in the DST scores (F=1.144, P=0.309).
Table 5 shows the differences between participants in different demographic categories in terms of the total digit span and the longest digit sequence of two subtests of the DST. As seen, participants of five age groups have significant differences in all four DST scores (the fDST longest digit sequence: F=2.664, P=0.023; the fDST total digit span: 3.859, P=0.002; the bDST longest digit sequence: F=2.663, P =0.023 and the bDST total digit span: F=3.354, P=0.004). Women and men have a significant difference in the bDST longest sequence (F=4.536, P=0.034), which according to Table 1, Mean±SD of men (4.65±1.23) have a higher score than Mean±SD of women (4.56±1.30). However, there was no difference in the fDST total digit span (F=0.190, P=0.663), the fDST longest digit sequence (F=0.104, P=0.747) and the bDST total digit span (F=3.7, P=0.056) among women and men. Participants with academic education differed from those with sub-academic education in terms of all scores (the fDST longest digit sequence: F=8.109, P=0.005; the fDST total digit span: F=11.493, P=0.001; the bDST longest digit sequence: F=17.551, P=0.001 and the bDST total digit span: F=20.856, P=0.000). According to Table 1, participants with an academic education (the fDST Mean±SD longest digit sequence: 5.60±1.14; the fDST Mean±SD total digit span: 8.31±1.98; the bDST Mean±SD longest digit sequence: 4.70±1.23; and the bDST Mean±SD total digit span: 6.38±2.10) in all scores were higher than those with sub-academic education (the fDST Mean±SD longest digit sequence: 5.17±1.07; the fDST Mean±SD total digit span: 7.28±1.64; the bDST Mean±SD longest digit sequence: 4.10±1.09; and the bDST Mean±SD total digit span: 5.09±1.50). Men and women in different age groups also differed from each other in terms of the fDST longest sequence (F=2.382, P=0.039) and the bDST longest sequence (F=3.253, P=0.007). Also, the participants with academic education were different from those with sub-academic education in different age groups in terms of the bDST total digit span (F=3.17, P=0.009) and the bDST longest digit sequence (F=2.29, P=0.046).
Table 6 presents the results of the Tukey post hoc test to examine the differences in the DST scores in the age groups of participants. In both DST subtests, participants under 40 had significantly higher total digit span and longest digit sequence than older participants (P<0.05). However, participants aged 40 to 70 did not differ in this respect (P>0.05).
Discussion
In this study, we aimed to collect Iranian normative data on one of the most well-known and widely-used tests of working memory and attentional capacity. We also examined whether the three demographic variables of age, education, and gender affect the performance of normal people in the forward and backward subtests of DST. Our findings showed that age had a significant negative correlation with both fDST and bDST, which means that the performance in DST decreased with age. Unlike age, education had a significant positive correlation with both subtests, which means that the performance in DST increases with increasing education level. However, there was no significant correlation between gender and DST scores. In addition, MANOVA showed a significant difference in DST scores between different age groups and education levels, with no difference between the two genders.
Our study demonstrated that the performance in DST as a measure of memory span and attentional capacity declines with age. The literature shows the significant effects of some demographic variables like age on different domains of cognitive functioning [41]. In particular, it has been demonstrated that aging is associated with performance decline in some cognitive capacities and functions [24, 41]. A study of 723 normal Chinese adult participants found that younger adults performed better on DST [41]. In another study of 164 individuals without cognitive complaints, age showed an inverse correlation with the scores obtained in DST, while education and gender did not have a significant relationship [31]. A decremental effect of age on DST performance at older ages has also been reported. A study of 3268 cognitively normal older adults found that increasing age is related to decreasing DST scores [24]. Also, in a study of 784 people aged 60-90 without serious neurological, medical and psychiatric complaints, DST performance decreased with older age [32].
Despite many studies favoring the decremental effect of aging on DST performance, some studies have not shown such an effect. In a sample of Spanish-speaking normal people over 55, age was not correlated to the DST performance [29]. Another study investigating the effect of increasing age on the cognitive functioning of 658 adults aged 60-84 found that increasing age did not affect DST performance [42]. In addition, in a study of 332 cognitively normal Spanish adults, no decremental effect of age was found [43]. This finding was repeated in two other studies on Hispanic adults aged 75-19 years [44] and 75-16 years [45]. In explaining the findings related to the lack of association between age and DST performance, some researchers have pointed out the simplicity of responding to DST stimuli and the difference in the research samples. It has been suggested that tests like DST are simpler than more complex tests like the symbol digit modalities test, and the effect of age is less visible [46].
According to our other finding, higher levels of education are associated with increased participants’ performance in DST. This finding is consistent with the results of many studies [43, 44, 41, 32, 24]. The relationship between education and DST performance is strong in many studies, and it is even observed without an association between age and DST scores. A study of 2574 Spanish-speaking participants found that the level of education is a stronger predictor of performance than age in both fDST and bDST [38]. In Spanish multicenter normative studies (NEURONORMA project) on 354 cognitively intact participants aged 50 to 90, although both age and education were related to performance on DST, the effect of education was greater than age [46]. In a sample of Spanish-speaking normal people over 55, age and gender were unrelated to fDST and bDST, and education was significantly associated with both modalities [22]. The effect of education on DST performance is so strong that even in people over 100 years of age (centenarians), this significant association has been observed [30].
In general, although some studies have documented the cognitive similarities of the two genders more than their differences [47], gender differences in various neuropsychological domains have been systematically reported in the literature [48]. However, our findings showed no association between DST performance and gender. The effect of gender on DST performance has been controversial in the literature [32]. Many studies have not reported such an effect [32, 43, 24]. A study of 723 normal Chinese adult participants found no significant difference between the two genders in DST performance [41]. Also, in a sample of Spanish-speaking normal people over 55 years old, gender was unrelated to fDST and bDST [22]. In another study, researchers examined the question of whether gender differences in working memory are related to the nature of the stimuli (verbal vs visuospatial). These researchers used forward and backward modalities of two working memory tests (Corsi block-tapping test with visuospatial stimuli and DST with verbal stimuli) to investigate this question. Their findings showed that both genders had no significant difference in fDST and bDST, while in the Corsi test, a significant difference was observed between them [49]. Men’s superiority in visuospatial processing over women has been proposed to explain such findings. This superiority can have an evolutionary origin [50]. More findings in support of this finding are obtained from studies that show that men have a significant advantage over women in tasks that require mental rotation [51].
A final point is worth noting here. One obvious benefit of providing normative data is that it can be used to interpret individual scores. Since most neuropsychological tests are standardized on normal populations, reporting the Mean±SD of the normative sample often allows a comparison between individual and normative scores. According to the commonly recommended rule in interpreting neuropsychological tests, 1.5 standard deviations below the normative mean indicate that a person’s performance was worse than approximately 93.3% of the normative sample. According to this rule, -1.5, -1.7, -2.0, -2.5 and -3.0 standard deviations below the normative mean will indicate mild, mild to moderate, moderate, severe and most severe levels of impairment, respectively [52].
Conclusion
In sum, our study, in addition to providing normative data for the well-known and widely-used measure of attention and working memory, the DST, showed that the two demographic variables of age and education significantly correlate with the fDST and bDST modalities. In contrast, gender did not show such an association. Considering the rapid aging of the population in Iran and the need for neuropsychological tools for diagnosis, treatment, prevention, and rehabilitation, our results help clinicians interpret the results of neuropsychological tests more accurately and reduce the possibility of false diagnoses of cognitive impairment. The findings of our study emphasize the importance of clinicians’ access to appropriate normative data for the Iranian population.
Limitations and future research
There are several limitations in our study. First, the education level of most participants in the study was higher than the diploma, and there were very few participants with an education lower than a diploma. The presence of equal or relatively equal proportions of participants with different levels of education in future studies can help to generalize the obtained results. Second, the sample used in our study was relatively small. This sample size may not be enough to generalize the results to the healthy Iranian population. It is recommended that a larger sample be used in future studies to collect normative data on the Iranian population. Third, the research sample was analyzed based on the three variables of age, sex, and education without differentiating them based on ethnicity, race, socioeconomic status and cultural factors. Considering the variables of ethnicity, race, socioeconomic status, and cultural factors may be important to collect normative data. Classifying the research sample based on the above variables in future studies can increase our understanding of the effect of different demographic variables on cognitive performance. It can provide more accurate normative data for clinical and research settings.
Ethical Considerations
Compliance with ethical guidelines
All study procedures were in compliance with the ethical guidelines of the 2013 Declaration of Helsinki. The present study was approved by the Ethics Committee of the National Institute for Medical Research Development (NIMAD) (Code: IR NIMAD REC.1396.319). Participation in the study was voluntary and written consent was obtained from all participants.
Funding
This study was financially supported by the Iranian National Institute for Medical Research Development (NIMAD) (Grant No.: 962550).
Authors contributions
Conceptualization, validation and methodology: Minoo Sisakhti and Seyed Amir Hossein Batouli; Statistical analysis: Hassan Farrahi and Elaheh Delazar; Supervision, investigation and data curation: Minoo Sisakhti and Seyed Amir Hossein Batouli; Writing the original draft: Hassan Farrahi and Elaheh Delazar; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors would like to thank all the participants in the various stages of the present study, from interviewing and testing to structural and functional imaging.
References
- Andrewes D. Neuropsychology: From theory to practice. London: Psychology Press; 2015. [Link]
- Rabin LA, Paolillo E, Barr WB. Stability in Test-Usage practices of clinical neuropsychologists in the United States and Canada over a 10-year period: A follow-up survey of INS and NAN Members. Arch Clin Neuropsychol. 2016; 31(3): 206-30. [DOI:10.1093/arclin/acw007] [PMID]
- Makowski D, Chen A, Larsen RR, Boyle GJ, Lilienfeld SO. Clinical neuropsychology in the era of neuroimaging. In: Boyle GJ, editor. The SAGE Handbook of clinical neuropsychology: clinical neuropsychological disorders. California: SAGE Publications Inc; 2023. [Link]
- Donders J. The incremental value of neuropsychological assessment: A critical review. Clin Neuropsychol. 2020; 34(1):56-87. [DOI:10.1080/13854046.2019.1575471] [PMID]
- Casaletto KB, Heaton RK. Neuropsychological Assessment: Past and future. J Int Neuropsychol Soc. 2017; 23(9-10):778-90. [DOI:10.1017/S1355617717001060] [PMID] [PMCID]
- Lezak MD. Neuropsychological assessment. Oxford: Oxford University Press; 2004. [Link]
- Sherman E, Hrabok M. A compendium of neuropsychological tests: Fundamentals of neuropsychological assessment and test reviews for clinical practice. Oxford: Oxford University Press; 2023. [Link]
- Harvey PD. Domains of cognition and their assessment. Dialogues Clin Neurosci. 2019; 21(3):227-37. [DOI:10.31887/DCNS.2019.21.3/pharvey] [PMID] [PMCID]
- Groth-Marnat G, Baker S. Digit Span as a measure of everyday attention: A study of ecological validity. Percept Mot Skills. 2003; 97(3 Pt 2):1209-18. [DOI:10.2466/pms.2003.97.3f.1209] [PMID]
- Tamez E, Myerson J, Morris L, White DA, Baum C, Connor LT. Assessing executive abilities following acute stroke with the trail making test and digit span. Behav Neurol. 2011; 24(3):177-85. [PMID]
- Hilbert S, Nakagawa TT, Puci P, Zech A, Bühner M. The digit span backwards task: Verbal and visual cognitive strategies in working memory assessment. Eur J Psychol Assess. 2014; 31(3), 174-180. [Link]
- Gardner RA. Digits forward and digits backward as two separate tests: Normative data on 1567 school children. J Clin Child Adolesc Psychol. 1981; 10(2):131-5. [Link]
- Groth-Marnat G. Handbook of psychological assessment. New York: John Wiley & Sons; 2009. [Link]
- Kiewel NA, Wisdom NM, Bradshaw MR, Pastorek NJ, Strutt AM. A retrospective review of digit span-related effort indicators in probable Alzheimer’s disease patients. Clin Neuropsychol. 2012; 26(6):965-74. [PMID]
- Welsh AJ, Bender HA, Whitman LA, Vasserman M, Macallister WS. Clinical utility of reliable digit span in assessing effort in children and adolescents with epilepsy. Arch Clin Neuropsychol. 2012; 27(7):735-41. [DOI:10.1093/arclin/acs063] [PMID]
- Asgari M, Gale R, Wild K, Dodge H, Kaye J. Automatic assessment of cognitive tests for differentiating mild cognitive impairment: A proof of concept study of the digit span task. Curr Alzheimer Res. 2020; 17(7):658-66. [DOI:10.2174/1567205017666201008110854] [PMID] [PMCID]
- Conklin HM, Curtis CE, Katsanis J, Iacono WG. Verbal working memory impairment in schizophrenia patients and their first-degree relatives: Evidence from the digit span task. Am J Psychiatry. 2000; 157(2):275-7. [DOI:10.1176/appi.ajp.157.2.275] [PMID]
- Kerruish L, Cheng AS, Ting KH, Liu KP. Exploring the sustained and divided attention of novice versus experienced drivers. Transp Res Interdiscip Perspect. 2022; 16:100702. [DOI:10.1016/j.trip.2022.100702]
- Shura RD, Martindale SL, Taber KH, Higgins AM, Rowland JA. Digit Span embedded validity indicators in neurologically-intact veterans. Clin Neuropsychol. 2020; 34(5):1025-37. [DOI:10.1080/13854046.2019.1635209] [PMID]
- Minoretti P, Santiago Sáez AS, García Martín ÁF, Liaño Riera M, Gómez Serrano M, Emanuele E. Mild depressive symptoms in airline pilots associated with impaired executive functions. Cureus. 2023; 15(7):e41616. [PMID]
- Kirkwood MW, Hargrave DD, Kirk JW. The value of the WISC-IV Digit Span subtest in detecting noncredible performance during pediatric neuropsychological examinations. Arch Clin Neuropsychol. 2011; 26(5): 377-84. [DOI:10.1093/arclin/acr040] [PMID]
- Dassanayake TL, Hewawasam C, Baminiwatta A, Ariyasinghe DI. Regression-based, demographically adjusted norms for Victoria Stroop Test, Digit Span, and Verbal Fluency for Sri Lankan adults. Clin Neuropsychol. 2021; 35(sup1):S32-49. [DOI:10.1080/13854046.2021.1973109] [PMID]
- Yoshimura T, Osaka M, Osawa A, Maeshima S. The classical backward digit span task detects changes in working memory but is unsuitable for classifying the severity of dementia. Appl Neuropsychol Adult. 2023; 30(5):528-34. [DOI:10.1080/23279095.2021.1961774] [PMID]
- Weintraub S, Salmon D, Mercaldo N, Ferris S, Graff-Radford NR, Chui H, et al. The Alzheimer’s Disease Centers’ Uniform Data Set (UDS): The neuropsychologic test battery. Alzheimer Dis Assoc Disord. 2009; 23(2):91-101. [DOI:10.1097/WAD.0b013e318191c7dd] [PMID] [PMCID]
- Freedman M, Leach L, Carmela Tartaglia M, Stokes KA, Goldberg Y, Spring R, et al. The Toronto Cognitive Assessment (TorCA): Normative data and validation to detect amnestic mild cognitive impairment. Alzheimers Res Ther. 2018; 10(1):65. [DOI:10.1186/s13195-018-0382-y]
- Ye S, Xie M, Yu X, Wu R, Liu D, Hu S, et al. The Chinese Brief Cognitive Test: Normative data stratified by gender, age and education. Front Psychiatry. 2022; 13:933642. [DOI:10.3389/fpsyt.2022.933642] [PMID] [PMCID]
- Fine EM, Kramer JH, Lui LY, Yaffe K; Study of Osteoporotic Fractures (SOF) Research Group. Normative data in women aged 85 and older: Verbal fluency, digit span, and the CVLT-II short form. Clin Neuropsychol. 2012; 26(1):18-30. [DOI:10.1080/13854046.2011.639310] [PMID] [PMCID]
- Dominguez JC, Phung TKT, de Guzman MFP, Fowler KC, Reandelar M Jr, Natividad B, et al. Determining Filipino Normative Data for a Battery of Neuropsychological Tests: The Filipino Norming Project (FNP). Dement Geriatr Cogn Dis Extra. 2019; 9(2):260-70. [DOI:10.1159/000500519] [PMID] [PMCID]
- Iñesta C, Oltra-Cucarella J, Bonete-López B, Calderón-Rubio E, Sitges-Maciá E. Regression-based normative data for independent and cognitively active Spanish older adults: Digit Span, letters and numbers, trail making test and symbol digit modalities test. Int J Environ Res Public Health. 2021; 18(19):9958. [DOI:10.3390/ijerph18199958] [PMID] [PMCID]
- Beker N, Sikkes SAM, Hulsman M, Schmand B, Scheltens P, Holstege H. Neuropsychological Test performance of cognitively healthy centenarians: Normative Data From the Dutch 100-Plus Study. J Am Geriatr Soc. 2019; 67(4):759-67. [DOI:10.1111/jgs.15729] [PMID] [PMCID]
- Abou-Mrad F, Chelune G, Zamrini E, Tarabey L, Hayek M, Fadel P. Screening for dementia in Arabic: Normative data from an elderly Lebanese sample. Clin Neuropsychol. 2017; 31(sup1):1-19. [DOI:10.1080/13854046.2017.1288270] [PMID]
- Choi HJ, Lee DY, Seo EH, Jo MK, Sohn BK, Choe YM, et al. A normative study of the digit span in an educationally diverse elderly population. Psychiatry Investig. 2014; 11(1):39-43. [DOI:10.4306/pi.2014.11.1.39] [PMID] [PMCID]
- Rabin LA, Nester CO, Barr WB. Current neuropsychological test usage practices. In: Boyle GJ, editor. The SAGE handbook of clinical neuropsychology: Clinical neuropsychological assessment and diagnosis. Los Angeles: SAGE Publications Inc., 2023. [DOI:10.4135/9781529789539.n2]
- Batouli SAH, Sisakhti M, Haghshenas S, Dehghani H, Sachdev P, Ekhtiari H, et al. Iranian Brain Imaging Database: A neuropsychiatric database of healthy brain. Basic Clin Neurosci. 2021; 12(1):115-32. [DOI:10.32598/bcn.12.1.1774.2] [PMID] [PMCID]
- Sisakhti M, Batouli SA, Farrahi H. The rey auditory verbal learning test: age-, gender- and education-related normative data for the Iranian Healthy Population. Front Biomed Technol. 2023; 10(3):308-20. [DOI:10.18502/fbt.v10i3.13162]
- Sisakhti M, Hosseini H, Batouli SA, Farrahi H. The benson complex figure test: Normative Data for the Healthy Iranian Population. Front Biomed Technol. 2024; 11(2):228-39. [DOI:10.18502/fbt.v11i2.15339]
- Cavaco S, Gonçalves A, Pinto C, Almeida E, Gomes F, Moreira I, et al. Auditory Verbal Learning Test in a large nonclinical Portuguese Population. Appl Neuropsychol Adult. 2015; 22(5):321-31. [DOI:10.1080/23279095.2014.927767] [PMID]
- Bezdicek O, Stepankova H, Moták L, Axelrod BN, Woodard JL, Preiss M, et al. Czech version of rey auditory verbal learning test: Normative data. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn. 2014;21(6):693-721. [DOI:10.1080/13825585.2013.865699] [PMID]
- Batouli SAH, Sisakhti M. Some points to consider in a task-based fMRI Study: A guideline for beginners. Front Biomed Technol. 2020; 7(1):52-73. [DOI:10.18502/fbt.v7i1.2725]
- Ostrosky-Solís F, Lozano A. Digit span: Effect of education and culture. Int J Psychol. 2006; 41(5):333-41. [DOI:10.1080/00207590500345724]
- Nichols ES, Wild CJ, Owen AM, Soddu A. Cognition across the Lifespan: Investigating age, sex, and other sociodemographic influences. Behav Sci (Basel). 2021; 11(4):51. [PMID]
- Harrington KD, Lim YY, Ames D, Hassenstab J, Rainey-Smith S, Robertson J, et al. Using robust normative data to investigate the neuropsychology of cognitive aging. Arch Clin Neuropsychol. 2017; 32(2):142-54. [DOI:10.1093/arclin/acw106] [PMID]
- Alegret M, Espinosa A, Vinyes-Junqué G, Valero S, Hernández I, Tárraga L, et al. Normative data of a brief neuropsychological battery for Spanish individuals older than 49. J Clin Exp Neuropsychol. 2012; 34(2):209-19. [DOI:10.1080/13803395.2011.630652] [PMID] [PMCID]
- Zimmermann N, Cardoso CO, Trentini CM, Grassi-Oliveira R, Fonseca RP. Brazilian preliminary norms and investigation of age and education effects on the Modified Wisconsin Card Sorting Test, Stroop Color and Word test and Digit Span test in adults. Dement Neuropsychol. 2015; 9(2):120-7. [DOI:10.1590/1980-57642015DN92000006] [PMID] [PMCID]
- Pontón MO, Satz P, Herrera L, Ortiz F, Urrutia CP, Young R, et al. Normative data stratified by age and education for the Neuropsychological Screening Battery for Hispanics (NeSBHIS): Initial report. J Int Neuropsychol Soc. 1996; 2(2):96-104. [DOI:10.1017/S1355617700000941] [PMID]
- Peña-Casanova J, Quiñones-Ubeda S, Quintana-Aparicio M, Aguilar M, Badenes D, Molinuevo JL, et al. Spanish Multicenter Normative Studies (NEURONORMA Project): Norms for verbal span, visuospatial span, letter and number sequencing, trail making test, and symbol digit modalities test. Arch Clin Neuropsychol. 2009; 24(4):321-41. [DOI:10.1093/arclin/acp038]
- Hyde JS. The gender similarities hypothesis. Am Psychol. 2005; 60(6):581-92. [PMID]
- Hyde JS. Gender similarities and differences. Annu Rev Psychol. 2014; 65:373-98. [PMID]
- Voyer D, Voyer SD, Saint-Aubin J. Sex differences in visual-spatial working memory: A meta-analysis. Psychon Bull Rev. 2017; 24(2):307-34. [DOI:10.3758/s13423-016-1085-7] [PMID]
- Piccardi L, D’Antuono G, Marin D, Boccia M, Ciurli P, Incoccia C, et al. New evidence for gender differences in performing the Corsi test but not the digit span: Data from 208 individuals. Psychol Stud. 2019; 64:411-9. [DOI:10.1007/s12646-019-00512-3]
- Barel E, Tzischinsky O. Age and sex differences in verbal and visuospatial abilities. Adv Cogn Psychol. 2018; 2(14):51-61. [DOI:10.5709/acp-0238-x] [PMID] [PMCID]
- Rahe M, Ruthsatz V, Quaiser-Pohl C. Influence of the stimulus material on gender differences in a mental-rotation test. Psychol Res. 2021; 85(8):2892-9. [DOI:10.1007/s00426-020-01450-w] [PMID]
Type of Study: Research |
Subject:
General
Received: 2024/02/27 | Accepted: 2024/05/6 | Published: 2024/07/7
Received: 2024/02/27 | Accepted: 2024/05/6 | Published: 2024/07/7
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
