Sat, May 18, 2024
Volume 10, Issue 1 (Winter 2024)
Caspian J Neurol Sci 2024, 10(1): 68-76 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Reihanian Z, Ashraf A, Mashategan M, Eftekhari B, Pourhabibi Z, Zaresharifi N. Changes in Serum Analytics and Biochemical Urinary Parameters Following Brain Tumor Operation. Caspian J Neurol Sci 2024; 10 (1) :68-76
URL: http://cjns.gums.ac.ir/article-1-692-en.html
URL: http://cjns.gums.ac.ir/article-1-692-en.html
Zoheir Reihanian1 

 , Ali Ashraf2 , Malihe Mashategan2 , Behrad Eftekhari3 , Zahra Pourhabibi4 , Nooshin Zaresharifi * 5
, Ali Ashraf2 , Malihe Mashategan2 , Behrad Eftekhari3 , Zahra Pourhabibi4 , Nooshin Zaresharifi * 5
, Ali Ashraf2 , Malihe Mashategan2 , Behrad Eftekhari3 , Zahra Pourhabibi4 , Nooshin Zaresharifi * 5
1- Department of Neurosurgery, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
2- Clinical Research Development Unit of Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
3- Department of Medicine, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
4- Vice-Chancellorship of Research and Technology, Guilan University of Medical Sciences, Rasht, Iran.
5- Department of Pathology, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
2- Clinical Research Development Unit of Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
3- Department of Medicine, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
4- Vice-Chancellorship of Research and Technology, Guilan University of Medical Sciences, Rasht, Iran.
5- Department of Pathology, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 1317 kb]
(105 Downloads)
| Abstract (HTML) (239 Views)
Full-Text: (53 Views)
Introduction
Currently, non-communicable diseases are considered the leading cause of death in the world [1]. Malignancies are the most prominent cause of death among non-communicable diseases, accounting for about 6.9 million deaths in 2018 [2]. Particularly, 1.6% of all new cancer cases and 2.5% of cancer-related mortalities are related to nervous system tumors [3]. The incidence of central nervous system tumors has risen by 40% in the past 20 years, particularly in adults [4]. Compared to the most common malignancies, such as lung, breast, and prostate tumors, the rate of brain tumors is low. However, many of these tumors exhibit an aggressive clinical course due to direct brain tissue involvement, leading to a poor prognosis and short survival. Since there is no definitive treatment for patients suffering from such brain tumors, palliative therapy aiming to improve the patient’s life span and alleviate the patient’s symptoms becomes a priority [5]. The treatment plan for most brain tumor patients comprises surgical resection, followed by neo-adjuvant chemo/radiotherapy, if indicated [6], leading to some adverse complications like hemodynamic instability and neurotoxicity, impairing their quality of life [7].
Serum sodium level contributes to various biochemical pathways of the nervous system. Previous studies indicate that hyponatremia can have disruptive effects on the nervous system even in the absence of cerebral edema [8]. Furthermore, one of the disorders noticed by numerous researchers after brain tumor operation is water and electrolyte disturbances, mainly hyponatremia. This condition can be seen in patients with brain tumors due to the damage of antidiuretic hormone (ADH) releasing neurons, called the syndrome of inappropriate antidiuretic hormone secretion (SIADH) [9]. Cerebral salt-wasting syndrome (CSWS) is another hyponatremia-causing condition in these patients. Although the exact mechanism of CSWS in these patients is unknown, releasing natriuretic peptides from damaged brain tissue may cause hyponatremia by affecting the kidneys [10]. Another phenomenon in these patients is suppressing the sympathetic nervous system, which can result in hyponatremia by impacting the kidneys [11].
Moreover, in patients with co-existing brain tumors and brain edema, releasing a variety of chemical mediators such as glutamate, histamine, arachidonic acid, free radicals, or free fatty acids causes brain edema, leading to nerve cell damage. Usual treatments of cerebral edema (e.g. hyperosmolar drugs (such as mannitol), hyperventilation, corticosteroid injection, and diuretics) can cause water and electrolyte imbalance, including hyponatremia [12]. However, the early and timely diagnosis of water and electrolyte disorders, especially sodium imbalance, can prevent unwanted complications [13]. Because a few studies have been done in this regard, we intended to assess the changes in serum levels of electrolytes and urinary parameters in patients with brain tumors during the first 12 hours after operation.
Materials and Methods
This cross-sectional study was performed on 168 patients with supratentorial brain tumors who underwent brain operation in Poursina Hospital, Rasht City, Iran, in 2020. Patients were selected via convenience sampling. Those with a history of renal dysfunction (including renal failure and dialysis), who expired during or immediately after the operation, and patients with craniopharyngioma, pituitary adenoma, or periventricular tumors (due to the direct effect on water and electrolyte status) were excluded from the study. The study parameters included the patient’s demographic and hemodynamic parameters (blood pressure and pulse rate), serum sodium, potassium, blood urea nitrogen (BUN), creatinine levels, urine specific gravity, and urine output. The parameters were measured immediately and 12 hours after operation. All laboratory parameters were analyzed in Poursina Hospital’s Laboratory. Also, the patients were examined immediately and 12 hours after the operation regarding the medications used, including IV serums (type, dosage, and duration of administration). Besides mannitol, normal saline (10 mL/kg/h) was also administered to all patients.
We analyzed the data using SPSS software, version 26. The quantitative variables are displayed as Mean±SD and the qualitative variables as frequency (percentage). We used the Kolmogorov-Smirnov test to check the assumptions of normality. Using the Wilcoxon test, the statistical differences between the study variables were compared immediately and 12 hours after operation. Using the Kruskal-Wallis test, the statistical differences between the investigated variables at different time points after the operation were analyzed according to age, operation duration, and tumor type. We also examined the differences in study parameters between the genders using the Mann-Whitney U test. P<0.05 were considered statistically significant.
Results
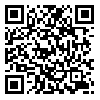
The baseline characteristics of the study population are presented in Table 1.
The Mean±SD age of the patients was 46.81±15.45 years, ranging from 9 to 80 years, with slender female predominance (54.8% over 45.2%). The Mean±SD operation duration was 323.99±67.91 minutes, ranging from 80 to 540 minutes. The Mean±SD mannitol usage was 347.56±63.63 mL, ranging from 100 to 500 mL. The most prevalent tumors were oligodendroglioma (32.1%), glioblastoma (25.0%), and meningioma (22.0%).
Regarding the laboratory parameters during the first 12 hours post-operation, the Mean±SD serum sodium levels were 139.70±5.60 meq/L and 140.34±6.23 meq/L (P=0.002), respectively; the Mean±SD serum potassium levels were 3.88±0.49 meq/L and 3.78±0.28 meq/L, (P=0.017), respectively, and the mean serum BUN values were 17.46±6.92 and 18.41±6.40 mg/dL (P=0.001), respectively. There was a significant increase in urinary output from 1043.70±455.00 mL to 1967.50±661.10 mL (P=0.008) and urine specific gravity from 1.010±0.007 to 1.012±0.008 (P=0.011). At the same time, the serum creatinine level changes remained insignificant (1.18±2.08 mg/dL versus 1.17±2.08 mg/dL, P=0.787).
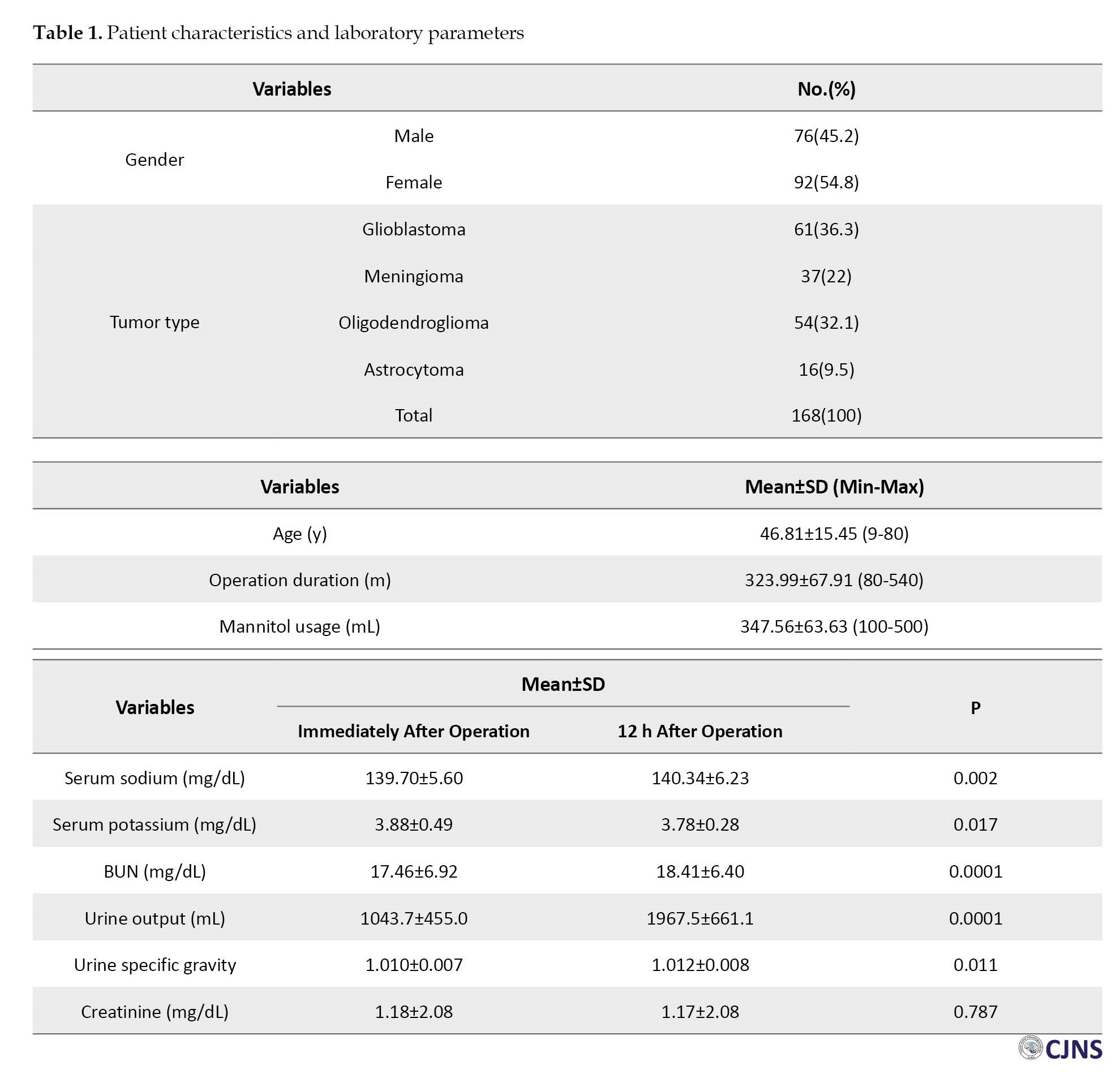
Table 2 presents age-adjusted serum analytics changes; an increase in serum sodium level was evident in ages over 40, while the decrease in serum potassium level occurred in patients younger than 40.
Additionally, serum BUN level alteration was significant in those under 60; however, serum creatinine levels remained unaffected between the ages of 40 and 60. The observed change in urine output was independent of the patient’s age.
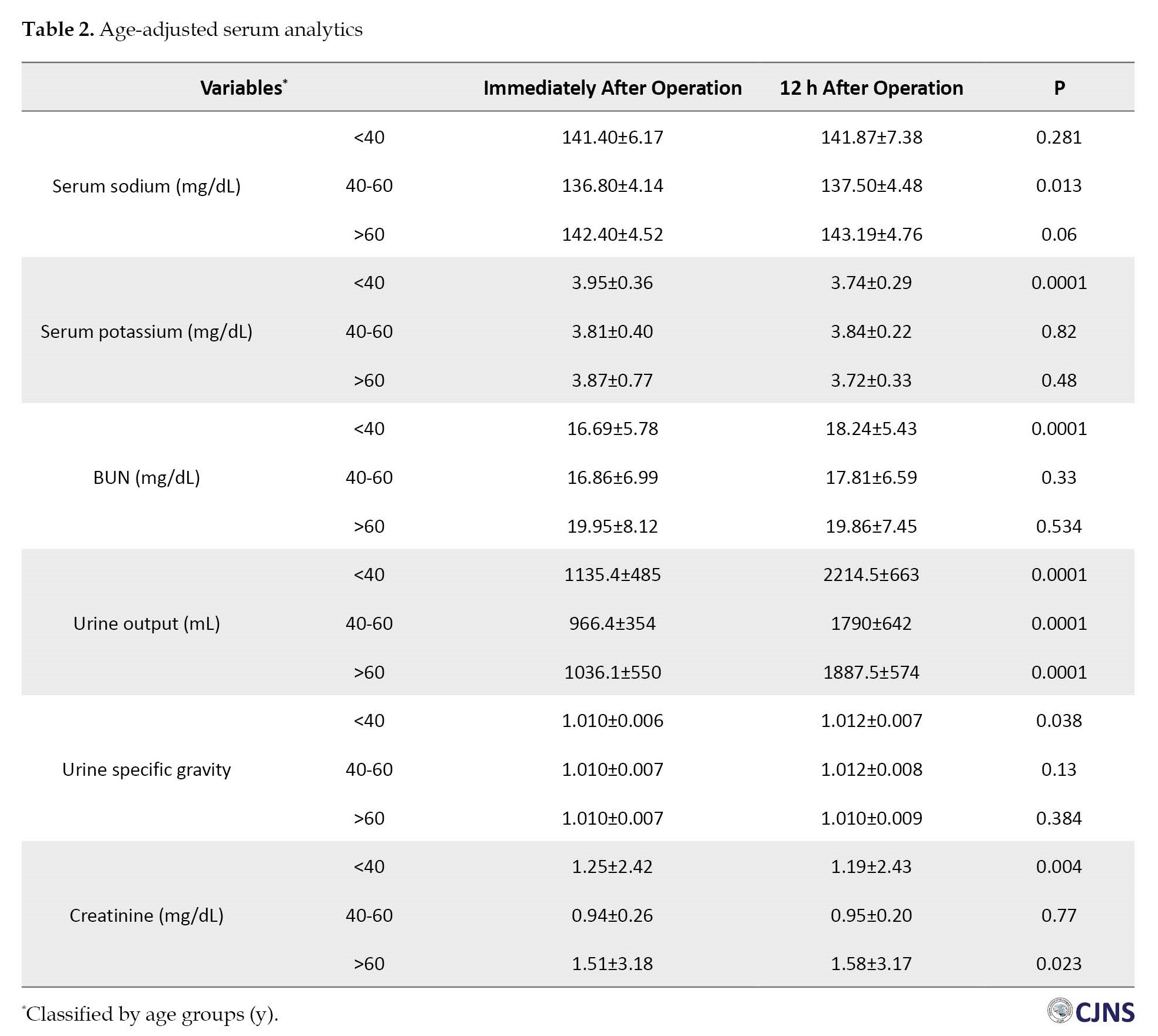
According to Table 3, the change in serum sodium and creatinine levels is associated with the male gender.
In contrast, the difference in serum potassium levels correlates more with the female gender. Urinary output and serum BUN levels change occurred equally in both genders.
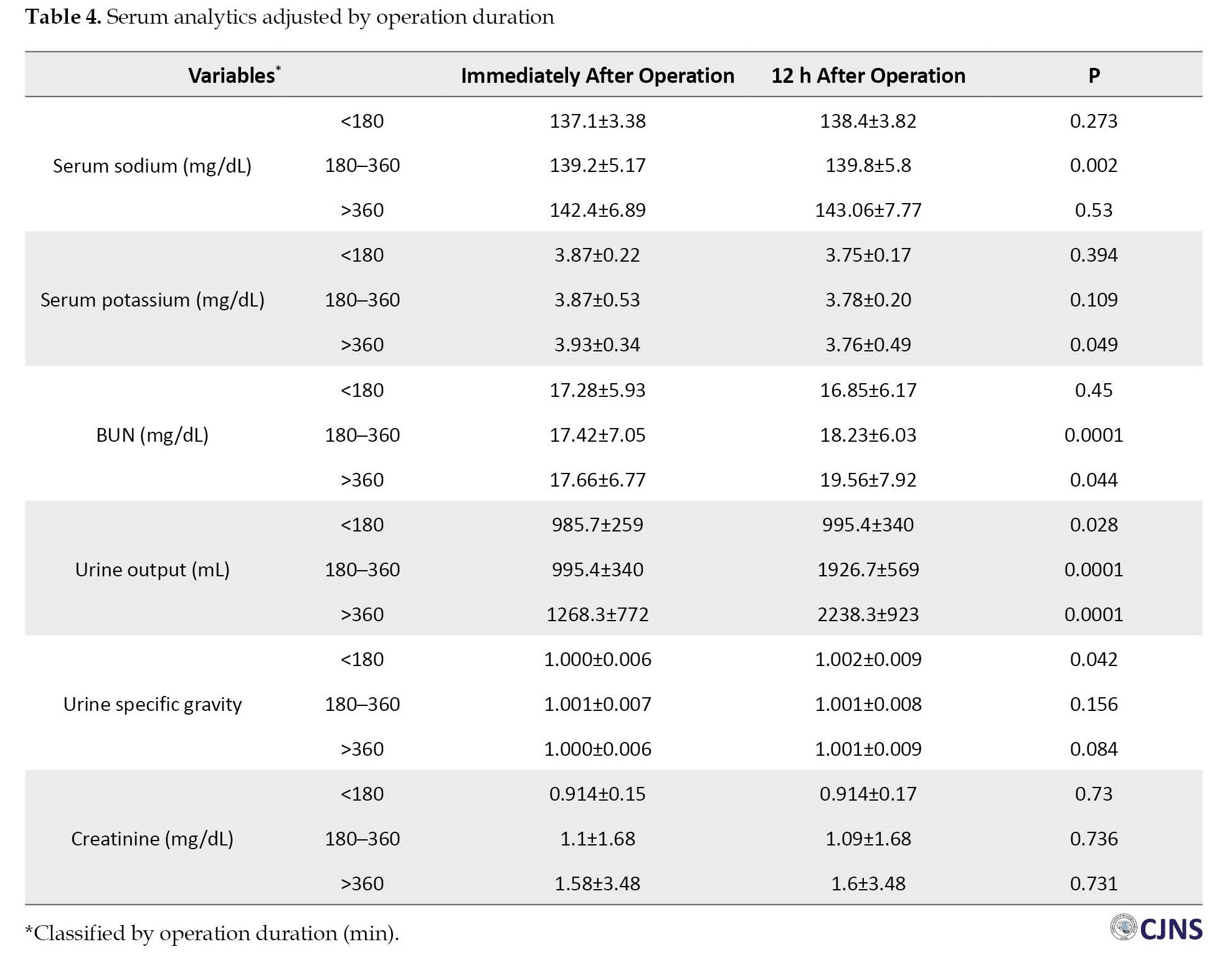
Table 4 presents that the duration of operation was also directly associated with the changes in serum potassium and BUN levels; the difference in serum sodium level was significant in a 180 to 360 min operation period, though the changes in serum creatinine happened independently from the operation duration.
As indicated in Table 5, the changes in serum BUN and potassium analytics were linked to high-dose mannitol intake, and serum sodium level alteration was found in patients with a 300 to 450 mL dose of mannitol.

The change in serum creatinine level was independent of the mannitol dosage.
Furthermore, the tumor type significantly affected the post-operative changes in laboratory indices (Table 6).

For example, oligodendroglioma and glioblastoma tumors showed significant changes in serum sodium and BUN levels; conversely, no significant changes were detected in serum potassium and creatinine levels regarding tumor type.
Discussion
Alterations in fluid and electrolytes soon after major operations such as craniotomy for brain tumors are expected owing to various causes, like diabetes insipidus, cerebral salt-wasting syndrome, and improper secretion of antidiuretic hormone. These changes mainly occur within the normal range and, if not so, are eventually reversible. Therefore, additional treatment may not be needed. On the other hand, in some cases, the extreme changes require precise management to reestablish the patient’s normal hemodynamic condition.
In this study, we observed an increase in serum sodium level within hours after brain tumor operation, correlated with male gender, older age, and the tumor types: Oligodendroglioma and glioblastoma. Although several studies have indicated the occurrence of acute hyponatremia following brain injury or tumor operation, this study revealed an acute post-operative increase regarding this serum element. The results of the Kiran et al. (2017) study indicated isolated hyponatremia in 11% and concurrent with diabetes insipidus in 9.2% of the sellar/suprasellar brain tumor patients undergone craniotomy [14]. Likewise, Kristof et al. (2009) prospectively studied the incidence, clinical manifestations, duration, and risk factors of water and electrolytes disorder following pituitary adenoma endoscopic operation; 21% of patients showed hyponatremia with 15.7% having coexistent diabetes insipidus [15]. Also, Belzer et al. (2014) investigated the duration and severity of hyponatremia after brain tumor operation in children in the United States. About 43% of patients experienced mild hyponatremia (ranging from 131 to 135 meq/L), 12% a more severe hyponatremia (serum sodium level of 130 or less meq/L), and 45% had normal sodium levels [16]. It can be concluded that hyponatremia is a highly probable complication following brain tumor operation, particularly in elderly male patients. However, other studies demonstrated hypernatremia after brain tumor operation, mainly due to salt excess from subsequent use of saline solutions and mannitol. The increased serum sodium level represents whole-body sodium accumulation and demands targeted hypernatremia treatment to achieve better post-operative outcomes and avoid hypernatremia-related complications such as focal intracerebral and subarachnoid hemorrhages and possibly irreversible neurologic damage.
Moreover, in line with the outcome of our study, Lili You et al. (2017), who investigated the prevalence of hypokalemia after operation for pituitary adenoma tumors, found that only in cases of ACTH-pituitary adenoma, the serum potassium level decrease was significant [17]. Since the drop in serum potassium level was observed mainly in patients with higher amounts of mannitol consumption, the leading cause of observed hypokalemia can be attributed to high doses of mannitol use. Similarly, in the Seo et al. study, the most notable finding was the high occurrence of hypokalemia observed during mannitol administration. Hypokalemia was observed in 22.0% of cases on the first day and constantly increased to 52.3% [18]. It should be noted that even slight changes in the serum potassium level can be associated with severe consequences owing to its narrow normal range, such as cardiac arrhythmias or severe muscle weakness resulting in respiratory failure and even death, which brings the essential need for vigilant monitoring of the element when coming upon major operations.
Besides, the present study revealed an increase in urinary output and urine specific gravity following brain tumor operation, both associated with diabetes insipidus caused by either the tumor or the operation [19]. Although a decrease in urinary output and urine specific gravity is expected immediately after a brain tumor resection, compensatory mechanisms gradually increase both indicators within a few hours post-operation.
Following brain tumor operation, no noticeable changes in serum creatinine levels were observed in this study; however, it should be evoked that kidney function changes following major operations may follow a more gradual course compared to electrolytes. Therefore, long-term follow-up is necessary to accurately trace such changes, specifically in patients with accompanying metastatic kidney disease.
Certain limitations of our study should be acknowledged. Firstly, only 168 patients with supratentorial brain tumors were included in our study. This moderate sample size restricts precise assessment of the effects of clinical characteristics of supratentorial tumors on serum hemodynamics. Secondly, our analysis was performed in Poursina Hospital, which mainly provides services for patients from northern Iran. It may further bring up a heterogenicity concerning the rest of the population in other regions. Further studies are needed to validate our findings, including a larger sample of more ethnically varied patients with supratentorial brain tumors. Also, we recommend further research to be done in the assessment of associations between brain tumor location with serum electrolyte profiles and the prognosis of patients who have undergone supratentorial operation and experienced post-operative electrolyte imbalance.
Conclusion
Based on the findings of our study, the changes in serum electrolytes and urinary laboratory parameters following brain tumor operation are predictable. In this regard, hypernatremia, hypokalemia, increase in urine volume, and specific gravity can be expected during the first 12 hours after the operation. Consequently, monitoring and managing a patient’s hemodynamics to track such changes during the very first hours after the operation will be crucial.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee at Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.361). The study process was in compliance with the ethical guidelines of the Declaration of Helsinki 2013.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, methodology, supervision, and project administration: Zoheir Reyhanian and Ali Ashraf; Data acquiation: Malihe Mashategan and Zahra Pourhabibi; Validation and revision: Nooshin Zaresharifi; Writing, preparation, review, and editing: Behrad Eftekhari.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We thanks Vice chancellorship of Research and technology of Guilan University of Medical Sciences and also thank the Clinical Research Development Unit of Poursina Hospital at Guilan University of Medical Sciences, the respectful faculty of Poursina Hospital, and the cooperative subjects of the study.
References
Currently, non-communicable diseases are considered the leading cause of death in the world [1]. Malignancies are the most prominent cause of death among non-communicable diseases, accounting for about 6.9 million deaths in 2018 [2]. Particularly, 1.6% of all new cancer cases and 2.5% of cancer-related mortalities are related to nervous system tumors [3]. The incidence of central nervous system tumors has risen by 40% in the past 20 years, particularly in adults [4]. Compared to the most common malignancies, such as lung, breast, and prostate tumors, the rate of brain tumors is low. However, many of these tumors exhibit an aggressive clinical course due to direct brain tissue involvement, leading to a poor prognosis and short survival. Since there is no definitive treatment for patients suffering from such brain tumors, palliative therapy aiming to improve the patient’s life span and alleviate the patient’s symptoms becomes a priority [5]. The treatment plan for most brain tumor patients comprises surgical resection, followed by neo-adjuvant chemo/radiotherapy, if indicated [6], leading to some adverse complications like hemodynamic instability and neurotoxicity, impairing their quality of life [7].
Serum sodium level contributes to various biochemical pathways of the nervous system. Previous studies indicate that hyponatremia can have disruptive effects on the nervous system even in the absence of cerebral edema [8]. Furthermore, one of the disorders noticed by numerous researchers after brain tumor operation is water and electrolyte disturbances, mainly hyponatremia. This condition can be seen in patients with brain tumors due to the damage of antidiuretic hormone (ADH) releasing neurons, called the syndrome of inappropriate antidiuretic hormone secretion (SIADH) [9]. Cerebral salt-wasting syndrome (CSWS) is another hyponatremia-causing condition in these patients. Although the exact mechanism of CSWS in these patients is unknown, releasing natriuretic peptides from damaged brain tissue may cause hyponatremia by affecting the kidneys [10]. Another phenomenon in these patients is suppressing the sympathetic nervous system, which can result in hyponatremia by impacting the kidneys [11].
Moreover, in patients with co-existing brain tumors and brain edema, releasing a variety of chemical mediators such as glutamate, histamine, arachidonic acid, free radicals, or free fatty acids causes brain edema, leading to nerve cell damage. Usual treatments of cerebral edema (e.g. hyperosmolar drugs (such as mannitol), hyperventilation, corticosteroid injection, and diuretics) can cause water and electrolyte imbalance, including hyponatremia [12]. However, the early and timely diagnosis of water and electrolyte disorders, especially sodium imbalance, can prevent unwanted complications [13]. Because a few studies have been done in this regard, we intended to assess the changes in serum levels of electrolytes and urinary parameters in patients with brain tumors during the first 12 hours after operation.
Materials and Methods
This cross-sectional study was performed on 168 patients with supratentorial brain tumors who underwent brain operation in Poursina Hospital, Rasht City, Iran, in 2020. Patients were selected via convenience sampling. Those with a history of renal dysfunction (including renal failure and dialysis), who expired during or immediately after the operation, and patients with craniopharyngioma, pituitary adenoma, or periventricular tumors (due to the direct effect on water and electrolyte status) were excluded from the study. The study parameters included the patient’s demographic and hemodynamic parameters (blood pressure and pulse rate), serum sodium, potassium, blood urea nitrogen (BUN), creatinine levels, urine specific gravity, and urine output. The parameters were measured immediately and 12 hours after operation. All laboratory parameters were analyzed in Poursina Hospital’s Laboratory. Also, the patients were examined immediately and 12 hours after the operation regarding the medications used, including IV serums (type, dosage, and duration of administration). Besides mannitol, normal saline (10 mL/kg/h) was also administered to all patients.
We analyzed the data using SPSS software, version 26. The quantitative variables are displayed as Mean±SD and the qualitative variables as frequency (percentage). We used the Kolmogorov-Smirnov test to check the assumptions of normality. Using the Wilcoxon test, the statistical differences between the study variables were compared immediately and 12 hours after operation. Using the Kruskal-Wallis test, the statistical differences between the investigated variables at different time points after the operation were analyzed according to age, operation duration, and tumor type. We also examined the differences in study parameters between the genders using the Mann-Whitney U test. P<0.05 were considered statistically significant.
Results
The baseline characteristics of the study population are presented in Table 1.
The Mean±SD age of the patients was 46.81±15.45 years, ranging from 9 to 80 years, with slender female predominance (54.8% over 45.2%). The Mean±SD operation duration was 323.99±67.91 minutes, ranging from 80 to 540 minutes. The Mean±SD mannitol usage was 347.56±63.63 mL, ranging from 100 to 500 mL. The most prevalent tumors were oligodendroglioma (32.1%), glioblastoma (25.0%), and meningioma (22.0%).
Regarding the laboratory parameters during the first 12 hours post-operation, the Mean±SD serum sodium levels were 139.70±5.60 meq/L and 140.34±6.23 meq/L (P=0.002), respectively; the Mean±SD serum potassium levels were 3.88±0.49 meq/L and 3.78±0.28 meq/L, (P=0.017), respectively, and the mean serum BUN values were 17.46±6.92 and 18.41±6.40 mg/dL (P=0.001), respectively. There was a significant increase in urinary output from 1043.70±455.00 mL to 1967.50±661.10 mL (P=0.008) and urine specific gravity from 1.010±0.007 to 1.012±0.008 (P=0.011). At the same time, the serum creatinine level changes remained insignificant (1.18±2.08 mg/dL versus 1.17±2.08 mg/dL, P=0.787).
Table 2 presents age-adjusted serum analytics changes; an increase in serum sodium level was evident in ages over 40, while the decrease in serum potassium level occurred in patients younger than 40.
Additionally, serum BUN level alteration was significant in those under 60; however, serum creatinine levels remained unaffected between the ages of 40 and 60. The observed change in urine output was independent of the patient’s age.
According to Table 3, the change in serum sodium and creatinine levels is associated with the male gender.
In contrast, the difference in serum potassium levels correlates more with the female gender. Urinary output and serum BUN levels change occurred equally in both genders.
Table 4 presents that the duration of operation was also directly associated with the changes in serum potassium and BUN levels; the difference in serum sodium level was significant in a 180 to 360 min operation period, though the changes in serum creatinine happened independently from the operation duration.
As indicated in Table 5, the changes in serum BUN and potassium analytics were linked to high-dose mannitol intake, and serum sodium level alteration was found in patients with a 300 to 450 mL dose of mannitol.
The change in serum creatinine level was independent of the mannitol dosage.
Furthermore, the tumor type significantly affected the post-operative changes in laboratory indices (Table 6).
For example, oligodendroglioma and glioblastoma tumors showed significant changes in serum sodium and BUN levels; conversely, no significant changes were detected in serum potassium and creatinine levels regarding tumor type.
Discussion
Alterations in fluid and electrolytes soon after major operations such as craniotomy for brain tumors are expected owing to various causes, like diabetes insipidus, cerebral salt-wasting syndrome, and improper secretion of antidiuretic hormone. These changes mainly occur within the normal range and, if not so, are eventually reversible. Therefore, additional treatment may not be needed. On the other hand, in some cases, the extreme changes require precise management to reestablish the patient’s normal hemodynamic condition.
In this study, we observed an increase in serum sodium level within hours after brain tumor operation, correlated with male gender, older age, and the tumor types: Oligodendroglioma and glioblastoma. Although several studies have indicated the occurrence of acute hyponatremia following brain injury or tumor operation, this study revealed an acute post-operative increase regarding this serum element. The results of the Kiran et al. (2017) study indicated isolated hyponatremia in 11% and concurrent with diabetes insipidus in 9.2% of the sellar/suprasellar brain tumor patients undergone craniotomy [14]. Likewise, Kristof et al. (2009) prospectively studied the incidence, clinical manifestations, duration, and risk factors of water and electrolytes disorder following pituitary adenoma endoscopic operation; 21% of patients showed hyponatremia with 15.7% having coexistent diabetes insipidus [15]. Also, Belzer et al. (2014) investigated the duration and severity of hyponatremia after brain tumor operation in children in the United States. About 43% of patients experienced mild hyponatremia (ranging from 131 to 135 meq/L), 12% a more severe hyponatremia (serum sodium level of 130 or less meq/L), and 45% had normal sodium levels [16]. It can be concluded that hyponatremia is a highly probable complication following brain tumor operation, particularly in elderly male patients. However, other studies demonstrated hypernatremia after brain tumor operation, mainly due to salt excess from subsequent use of saline solutions and mannitol. The increased serum sodium level represents whole-body sodium accumulation and demands targeted hypernatremia treatment to achieve better post-operative outcomes and avoid hypernatremia-related complications such as focal intracerebral and subarachnoid hemorrhages and possibly irreversible neurologic damage.
Moreover, in line with the outcome of our study, Lili You et al. (2017), who investigated the prevalence of hypokalemia after operation for pituitary adenoma tumors, found that only in cases of ACTH-pituitary adenoma, the serum potassium level decrease was significant [17]. Since the drop in serum potassium level was observed mainly in patients with higher amounts of mannitol consumption, the leading cause of observed hypokalemia can be attributed to high doses of mannitol use. Similarly, in the Seo et al. study, the most notable finding was the high occurrence of hypokalemia observed during mannitol administration. Hypokalemia was observed in 22.0% of cases on the first day and constantly increased to 52.3% [18]. It should be noted that even slight changes in the serum potassium level can be associated with severe consequences owing to its narrow normal range, such as cardiac arrhythmias or severe muscle weakness resulting in respiratory failure and even death, which brings the essential need for vigilant monitoring of the element when coming upon major operations.
Besides, the present study revealed an increase in urinary output and urine specific gravity following brain tumor operation, both associated with diabetes insipidus caused by either the tumor or the operation [19]. Although a decrease in urinary output and urine specific gravity is expected immediately after a brain tumor resection, compensatory mechanisms gradually increase both indicators within a few hours post-operation.
Following brain tumor operation, no noticeable changes in serum creatinine levels were observed in this study; however, it should be evoked that kidney function changes following major operations may follow a more gradual course compared to electrolytes. Therefore, long-term follow-up is necessary to accurately trace such changes, specifically in patients with accompanying metastatic kidney disease.
Certain limitations of our study should be acknowledged. Firstly, only 168 patients with supratentorial brain tumors were included in our study. This moderate sample size restricts precise assessment of the effects of clinical characteristics of supratentorial tumors on serum hemodynamics. Secondly, our analysis was performed in Poursina Hospital, which mainly provides services for patients from northern Iran. It may further bring up a heterogenicity concerning the rest of the population in other regions. Further studies are needed to validate our findings, including a larger sample of more ethnically varied patients with supratentorial brain tumors. Also, we recommend further research to be done in the assessment of associations between brain tumor location with serum electrolyte profiles and the prognosis of patients who have undergone supratentorial operation and experienced post-operative electrolyte imbalance.
Conclusion
Based on the findings of our study, the changes in serum electrolytes and urinary laboratory parameters following brain tumor operation are predictable. In this regard, hypernatremia, hypokalemia, increase in urine volume, and specific gravity can be expected during the first 12 hours after the operation. Consequently, monitoring and managing a patient’s hemodynamics to track such changes during the very first hours after the operation will be crucial.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee at Guilan University of Medical Sciences (Code: IR.GUMS.REC.1399.361). The study process was in compliance with the ethical guidelines of the Declaration of Helsinki 2013.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors contributions
Conceptualization, methodology, supervision, and project administration: Zoheir Reyhanian and Ali Ashraf; Data acquiation: Malihe Mashategan and Zahra Pourhabibi; Validation and revision: Nooshin Zaresharifi; Writing, preparation, review, and editing: Behrad Eftekhari.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
We thanks Vice chancellorship of Research and technology of Guilan University of Medical Sciences and also thank the Clinical Research Development Unit of Poursina Hospital at Guilan University of Medical Sciences, the respectful faculty of Poursina Hospital, and the cooperative subjects of the study.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68(6):394-424. [DOI:10.3322/caac.21492] [PMID]
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010; 60(5):277-300. [DOI:10.3322/caac.20073] [PMID]
- Kirkbride P, Tannock IF. Trials in palliative treatment-have the goal posts been moved? Lancet Oncol. 2008; 9(3):186- 7. [DOI:10.1016/S1470-2045(08)70041-X] [PMID]
- Preusser M, de Ribaupierre S, Wöhrer A, Erridge SC, Hegi M, Weller M, et al. Current concepts and management of glioblastoma. Ann Neurol. 2011; 70(1):9-21. [DOI:10.1002/ana.22425] [PMID]
- Abbasi Veldani N, pourandish Y, Mehrabi F. [The use of radiotherapy during operation in the treatment of brain tumors (systematic review)(Persian)]. Iran J Cancer Care. 2020; 1(4):39-47. [Link]
- Gankam Kengne F, Decaux G. Hyponatremia and the Brain. Kidney Int Rep. 2018; 3(1):24-35. [DOI:10.1016/j.ekir.2017.08.015] [PMID]
- Edate S, Albanese A. Management of electrolyte and fluid disorders after brain operation for pituitary/suprasellar tumors. Horm Res Paediatr. 2015; 83(5):293-301. [DOI:10.1159/000370065] [PMID]
- Momi J, Tang CM, Abcar AC, Kujubu DA, Sim JJ. Hyponatremia-what is cerebral salt wasting? Perm J. 2010; 14(2):62. [DOI:10.7812/TPP/08-066] [PMID]
- Yee AH, Burns JD, Wijdicks EF. Cerebral salt wasting: Pathophysiology, diagnosis, and treatment. Neurosurg Clin N Am. 2010; 21(2):339-52. [DOI:10.1016/j.nec.2009.10.011] [PMID]
- Jha SK. Cerebral edema and its management. Med J Armed Forces India. 2003; 59(4):326-31. [DOI:10.1016/S0377-1237(03)80147-8] [PMID]
- Segura Matute S, Balaguer Gargallo M, Cambra Lasaosa FJ, Zambudio Sert S, Martín Rodrigo JM, Palomeque Rico A. [Fluid and electrolyte disorders following surgery for brain tumors (Spanish)]. An Pediatr (Barc). 2007; 67(3):225-30.[DOI:10.1016/S1695-4033(07)70611-2] [PMID]
- Suman S, Kumar N, Singh Y, Kumar V, Yadav G, Gupta BK, et al. Evaluation of serum electrolytes in traumatic brain injury patients: prospective randomized observational study. J Anesth Crit Care Open Access. 2016; 5(3):00184. [DOI:10.15406/jaccoa.2016.05.00184]
- Kiran Z, Sheikh A, Momin SN, Majeed I, Awan S, Rashid O, et al. Sodium and water imbalance after sellar, suprasellar, and parasellar surgery. Endocr Pract. 2017; 23(3):309-17. [DOI:10.4158/EP161616.OR] [PMID]
- Kristof RA, Rother M, Neuloh G, Klingmüller D. Incidence, clinical manifestations, and course of water and electrolyte metabolism disturbances following transsphenoidal pituitary adenoma surgery: A prospective observational study: Clinical article. J Neurosurg. 2009; 111(3):555-62 [DOI:10.3171/2008.9.JNS08191] [PMID]
- Belzer JS, Williams CN, Riva-Cambrin J, Presson AP, Bratton SL. Timing, duration, and severity of hyponatremia following pediatric brain tumor surgery. Pediatr Crit Care Med. 2014; 15(5):456-63. [DOI:10.1097/PCC.0000000000000154] [PMID]
- You L, Li W, Chen T, Tang D, You J, Zhang X. A retrospective analysis of post-operative hypokalemia in pituitary adenomas after transsphenoidal surgery. PeerJ. 2017; 5:e3337 [DOI:10.7717/peerj.3337] [PMID]
- Seo W, Oh H. Alterations in serum osmolality, sodium, and potassium levels after repeated Mannitol administration. J Neurosci Nurs 2010; 42(4):201-7. [DOI:10.1097/JNN.0b013e3181e26b4a] [PMID]
Type of Study: Research |
Subject:
Special
Received: 2024/01/28 | Accepted: 2024/01/20 | Published: 2024/01/20
Received: 2024/01/28 | Accepted: 2024/01/20 | Published: 2024/01/20
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
