Sat, May 18, 2024
Volume 9, Issue 2 (Spring 2023)
Caspian J Neurol Sci 2023, 9(2): 120-128 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Norasteh A A, Balayi E, Zarei H. Functional Gait Assessment Tests in Elderly: A Systematic Review. Caspian J Neurol Sci 2023; 9 (2) :120-128
URL: http://cjns.gums.ac.ir/article-1-592-en.html
URL: http://cjns.gums.ac.ir/article-1-592-en.html



1- Physiotherapy Department, Faculty of Medicine, Guilan University of Medical Sciences, Guilan, Iran
2- Department of Corrective Exercise and Sports Injuries, Faculty of Physical Education and Sports Sciences, University of Guilan, Guilan, Iran
2- Department of Corrective Exercise and Sports Injuries, Faculty of Physical Education and Sports Sciences, University of Guilan, Guilan, Iran
Full-Text [PDF 1187 kb]
(433 Downloads)
| Abstract (HTML) (656 Views)
Full-Text: (137 Views)
Introduction
Aging is part of the biological process experienced by humans. Along with the growth of the elderly population globally, Iran’s population is also moving towards aging. It is estimated that by 2026, elderly Iranians will account for about 11% of the country’s total population [1]. One of the major challenges facing elderly care systems is the problem of falling among the elderly. Studies show that one in three older adults over the age of 65 experiences falls at least once a year with serious consequences [2]. Therefore, all elderly care systems sought to reduce or delay the number and frequency of falls in the elderly to increase active social participation of the elderly.
Aging leads to several significant changes such as increased reaction time, decreased balance, decreased neuromuscular coordination, decreased muscle strength, decreased flexibility, decreased posture control, and, consequently, increased risk of falls [3]. Therefore, studies use different tools and methods to examine each of these factors and predict the rate of falls in the elderly [4]. Using the results of these measurements, a series of interventions and detailed programs are developed to reduce the rate of falls in the elderly [5]. Therefore, the tools and methods used to study and predict the rate of falls in the elderly, including the study of gait in the elderly [6], are extremely important.
Gait is considered a basic skill to which most daily human motor activities are dedicated [6]. To control stature and maintain rhythm and stability while gait, a sophisticated control system is needed that can adapt to internal and external changes [7]. This control system depends on the coordination of sensory systems that detect the body’s position and movement, the visual environment, and the operating organs that produce postural and kinetic reactions [8]. In old age, this skill faces some problems including decreased gait speed, shorter stride length, increased double support time, decreased cadence, increased postural fluctuations, and greater variability of spatial-temporal parameters [9]. From this perspective, gait is considered an indicator to determine the degree to which the elderly can achieve independence in carrying out their daily activities [10]. Therefore, it is necessary to scrutinize this factor in the elderly because gait studies have been considered one of the main factors in predicting falls in the elderly [6].
The elderly population is growing. With age, the rate of falls in the elderly also increases, leading to several serious complications. Therefore, health systems must do their utmost to prevent falls among the elderly. One of the predictors of the risk of falls is the study of gait in the elderly, which requires appropriate methods. The reason is that the necessary interventions are made based on the results of this evaluation. Studies have used different methods to assess gait in the elderly. Gait in the elderly has been evaluated in two ways: the use of advanced equipment and functional tests [6]. The former increases the accuracy of measurements, while the latter is costly and cannot be applied anywhere. Due to the mobility problems of the elderly, it is better to use low-cost and applicable methods in any place, which do not require expertise to measure gait. One of these ubiquitous methods is functional gait assessment (FGA). Therefore, this study collects all FGAs used to evaluate the elderly for a general review of the tests and their functional characteristics. Therefore, the purpose of this review study is to evaluate FGA in the elderly.
Materials and Methods
Search strategies
This study conducted a comprehensive review of FGA in the elderly. For this purpose, searches were done in PubMed, Medline, Web of Science, ScienceDirect, Cochrane Central Register of Controlled Clinical Trials, Google Scholar, Scopus, Magiran, Irandoc, IranMedex, MedLib, and SID databases from 1996 to November 2020.
Keywords
A search was performed in databases using the following keywords: 1) Walk; Gait; Locomot; Ambulat; AND 2) Elder; Old; Older adult; Senescent; Senile; Aged; Gray; Geriatric; Age; Aging; AND 3) Functional tests; Physical examination; Functional performance tests; Lower extremity tests. The “AND” operator was used between the 3 keyword groups, while the “OR” operator was used within each keyword group. After collecting the search results, first, the titles were studied followed by the abstracts. If an article matched the inclusion and exclusion criteria, its results were used in the review study; otherwise, it was excluded. Based on the criteria and objectives of the research, 19 articles were selected after evaluation. All articles were provided in full text.
Exclusion and inclusion criteria
Inclusion criteria: In the first stage, the titles and abstracts of descriptive studies were screened with a focus on FGA in the elderly and their publication in Persian and English. Then, a research assistant independently reviewed the abstracts of the articles. The second step involved screening the entire text by a researcher concerning the release of the index (i.e. FGA in the elderly) and a specific target population (i.e. elderly). A senior researcher then checked the final list of selected papers to ensure that all papers aligned with the research objectives. A summary of the descriptive information was then collected by the research assistant and checked by the senior researcher. A sample table (Figure 1) was used to extract information about the target population, FGA in the elderly, and their results.
.jpg) Exclusion criteria: The exclusion criteria included articles that did not address the elderly statistical population, articles that did not well define the stages of a test, and articles that used rigorous laboratory tools, which are not classified as functional tests.
Exclusion criteria: The exclusion criteria included articles that did not address the elderly statistical population, articles that did not well define the stages of a test, and articles that used rigorous laboratory tools, which are not classified as functional tests.
Quality of evidence
The risk of bias was evaluated by both reviewers using Newcastle-Ottawa Quality Assessment Scale (NOS) [11]. Herzog et al.’s checklist for cross-sectional studies was employed [11]. Quality was assessed based on Herzog et al., as follows: Very Good Studies: 9-10 stars, Good Studies: 7-8 stars, Satisfactory Studies: 5-6 stars, Unsatisfactory Studies: 0-4 stars [11].
Data extraction
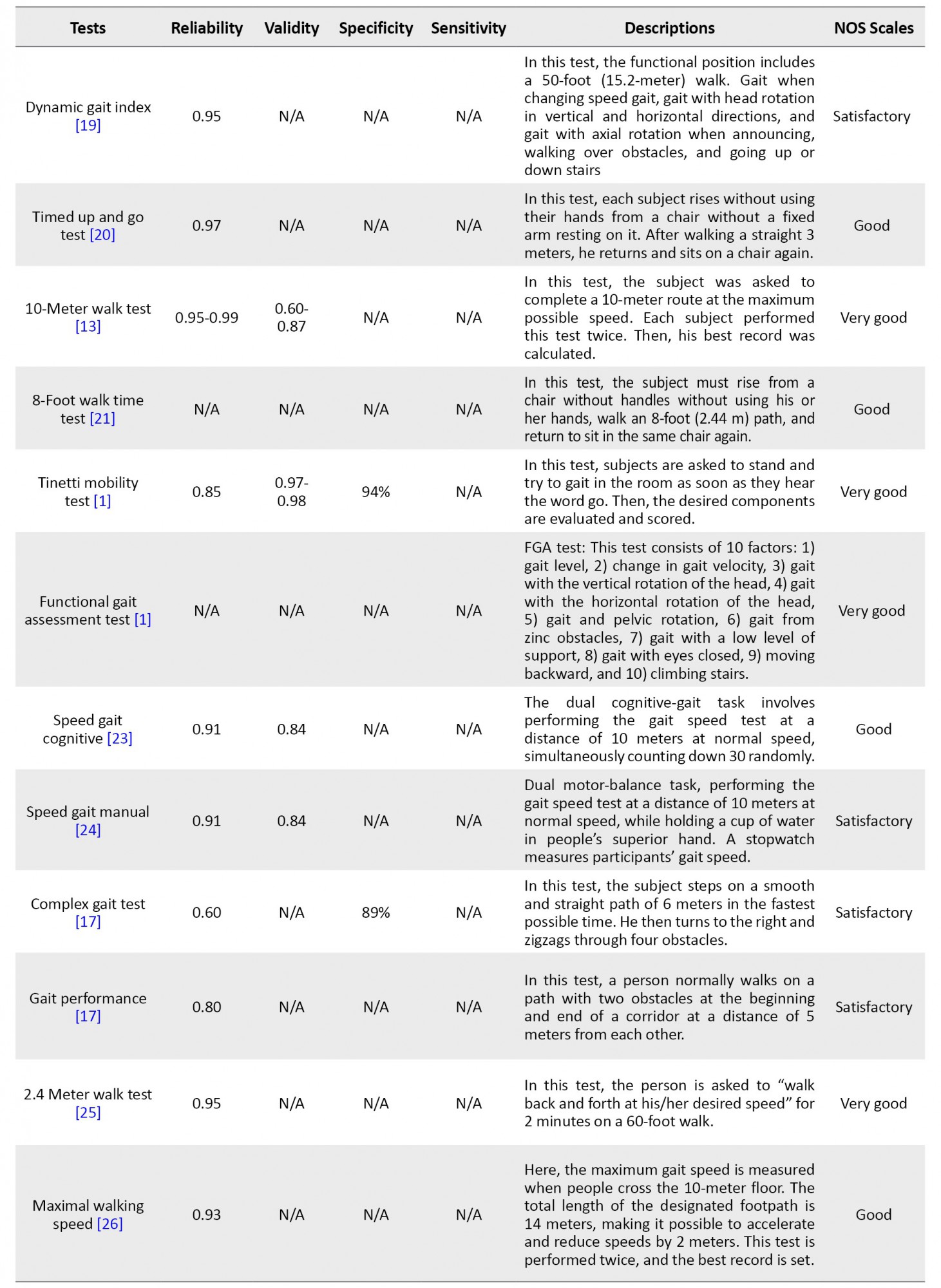
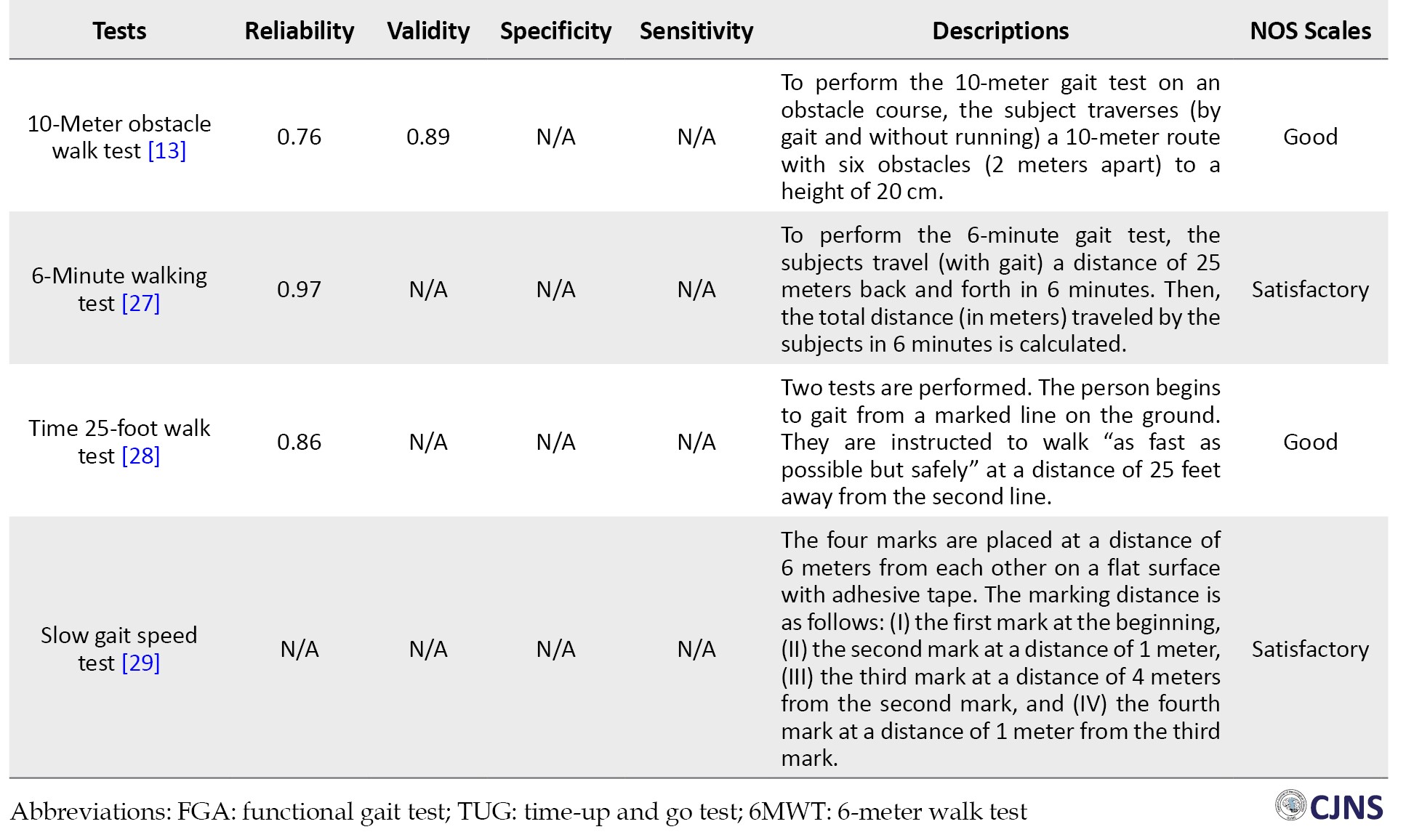
Data from studies were extracted independently by Researchers using some measures including the first reference and name of functional tests, validity, reliability, an explanation of how to evaluate and perform functional tests, and quality of evidence (Table 1).

Results
An electronic resource search yielded 367 titles. Furthermore, manually searching and reviewing the sources of articles gained 10 more titles. Following the removal of duplicate titles, 189 abstracts were identified for review. After reviewing the articles’ titles and abstracts, 145 articles were excluded, and 44 articles were selected to read the full text. After reviewing the articles’ full text, we selected and reported the results of 19 articles from 23 different tests, which studied FGA in the elderly (Table 1).
Based on the results of NOS, studies that were systematically reviewed had desirable qualities: 5 studies (22%) as very good (9-10 stars); 10 studies (44%) as good (7-8 stars), and 8 studies (34%) as satisfactory. Therefore, the studies that were systematically reviewed are of a very good to satisfactory quality. Results were shown in Table 1.
Discussion
This study aimed to evaluate FGA methods in the elderly. A review of the studies revealed that the studies used several methods to evaluate FGA in the elderly. In this review study, 19 articles were found from 23 multiple tests that attempted to examine FGA in the elderly. The features of these tests are discussed below.
An important factor examined in most FGAs in the elderly is gait assessment in the elderly speed [13, 21, 22, 26, 28]. Older people who take the test will score high in a short period, indicating that they are less prone to falls. Studies have examined the relationship between gait velocity and the risk of falling elderly [30, 31]. According to the results, the lower the gait speed in the elderly, the higher the risk of falls. Moreover, gait speed tests suitable for the elderly have been identified. Attempts have been made to answer the following questions: “Should tests be used in which the elderly are asked to walk at maximum speed or normal speed?” “Which of these factors best predicts the risk of falls in the elderly?” A study showed that both normal gait and gait factors with maximum speed could well predict the risk of falls in the elderly [32]. Therefore, in the case of gait in the elderly speed factor assessment tests, no distinction can be made between the tests that examined the maximum gait in the elderly rate and those that examined their normal gait rate. Both can predict the risk of falls in the elderly with approximately an equal probability.
Additionally, a 6-minute walking test [27] is designed to assess lower extremity muscle endurance in the elderly. In this test, the older the person who can walk, the more distance in 6 minutes and the higher the score, indicating a better physical condition of the elderly. Studies have evaluated the ability of the 6-minute walking test to predict the risk of falls in the elderly [33, 34]. The results showed that the 6-minute walking test could predict the risk of falls in the elderly with greater accuracy. It is also closely related to other physiological and psychological factors of the elderly. Therefore, it can be concluded that the 6-minute walking test is a practical test for assessing gait in the elderly. The results of this test can be used to evaluate the functional characteristics and risk of falls in the elderly.
Furthermore, among the FGA, several tests have examined gait by adding functional and cognitive tasks to the case [24, 25, 26, 27, 28, 29]. Several tasks were imposed on the elderly during gait to approximate the normal daily life of the elderly and to examine the elderly gait. These studies have shown that several other posture control factors may be involved in gait in the elderly and increase the risk of falls in the elderly. Therefore, these studies attempted to examine gait in the elderly by giving multiple tasks. Several studies have also investigated the effect of these tasks on gait in the elderly [35, 36, 37]. They concluded that multiple posture control factors could affect gait in the elderly, and consequently, increase the risk of falls in the elderly [38]. Studies have shown that the risk of falls in the elderly increases by adding task posture control during gait [39].
Therefore, it can be concluded that the purpose of designing these tests is to examine the effect of several different tasks during gait in the elderly. The results of this test can help accurately and correctly predict the physical condition and the risk of falls in the elderly.
Features of a valid functional test include validity, reliability, sensitivity, and high specificity. This review study examined FGA and found that validity and reliability were reported for most FGAs. However, few studies have addressed the sensitivity and specificity of FGA in the elderly. The sensitivity and specificity of tests were not reported for most FGAs. Sensitivity means that the number of people who fall is correctly identified, and specificity means that the number of people who do not fall is correctly identified. High sensitivity indicates that the test is suitable for screening.
On the other hand, high specificity indicates that the test is suitable for diagnosis. Therefore, studies should also specifically address the sensitivity and specificity of FGA in the elderly, as they help to more accurately analyze gait in the elderly functional tests. As a result, more accurate and appropriate interventions and programs can be developed following FGA measurements in the elderly.
This review study used a systematic search methodology but failed to quantify the articles. Although most articles taken from reputable international scientific-research journals are domestic and have an acceptable quality rating, care should be taken in generalizing their results. Moreover, although complete search strategies were used, only English and Persian articles were reviewed. There may be other related articles in other languages. Therefore, considering the mentioned limitations, future research should review the articles qualitatively.
Conclusion
Studies show that they treat FGA in the elderly using different methods and for different purposes. Studies to measure gait speed, normal gait, gait, and functional and cognitive tasks have helped measure functional gait in the elderly. Few studies have addressed the two main features of a valid test, sensitivity, and specificity. Studies should focus as much as possible on these test features in measuring FGA in the elderly.
Ethical Considerations
Compliance with ethical guidelines
Since this study is a review and does not require ethical approval, no university has been approved by the ethics committee. Also, the ethical principles in writing the article have been observed according to the instructions of the National Ethics Committee and the COPE regulations.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: All authors; Methodology and Investigation: Esmail Balaiy, Hamed Zarei; Supervision, Writing--original draft, Writing--review & editing: Ali Asghar Norasteh, Hamed Zarei; Funding acquisition: Esmail Balaiy; Resources: All author.
Conflict of interest
The authors report no conflict of interest.
Acknowledgements
The researchers thank the head of the Faculty of Physical Education, University of Guilan, Iran.
References
Aging is part of the biological process experienced by humans. Along with the growth of the elderly population globally, Iran’s population is also moving towards aging. It is estimated that by 2026, elderly Iranians will account for about 11% of the country’s total population [1]. One of the major challenges facing elderly care systems is the problem of falling among the elderly. Studies show that one in three older adults over the age of 65 experiences falls at least once a year with serious consequences [2]. Therefore, all elderly care systems sought to reduce or delay the number and frequency of falls in the elderly to increase active social participation of the elderly.
Aging leads to several significant changes such as increased reaction time, decreased balance, decreased neuromuscular coordination, decreased muscle strength, decreased flexibility, decreased posture control, and, consequently, increased risk of falls [3]. Therefore, studies use different tools and methods to examine each of these factors and predict the rate of falls in the elderly [4]. Using the results of these measurements, a series of interventions and detailed programs are developed to reduce the rate of falls in the elderly [5]. Therefore, the tools and methods used to study and predict the rate of falls in the elderly, including the study of gait in the elderly [6], are extremely important.
Gait is considered a basic skill to which most daily human motor activities are dedicated [6]. To control stature and maintain rhythm and stability while gait, a sophisticated control system is needed that can adapt to internal and external changes [7]. This control system depends on the coordination of sensory systems that detect the body’s position and movement, the visual environment, and the operating organs that produce postural and kinetic reactions [8]. In old age, this skill faces some problems including decreased gait speed, shorter stride length, increased double support time, decreased cadence, increased postural fluctuations, and greater variability of spatial-temporal parameters [9]. From this perspective, gait is considered an indicator to determine the degree to which the elderly can achieve independence in carrying out their daily activities [10]. Therefore, it is necessary to scrutinize this factor in the elderly because gait studies have been considered one of the main factors in predicting falls in the elderly [6].
The elderly population is growing. With age, the rate of falls in the elderly also increases, leading to several serious complications. Therefore, health systems must do their utmost to prevent falls among the elderly. One of the predictors of the risk of falls is the study of gait in the elderly, which requires appropriate methods. The reason is that the necessary interventions are made based on the results of this evaluation. Studies have used different methods to assess gait in the elderly. Gait in the elderly has been evaluated in two ways: the use of advanced equipment and functional tests [6]. The former increases the accuracy of measurements, while the latter is costly and cannot be applied anywhere. Due to the mobility problems of the elderly, it is better to use low-cost and applicable methods in any place, which do not require expertise to measure gait. One of these ubiquitous methods is functional gait assessment (FGA). Therefore, this study collects all FGAs used to evaluate the elderly for a general review of the tests and their functional characteristics. Therefore, the purpose of this review study is to evaluate FGA in the elderly.
Materials and Methods
Search strategies
This study conducted a comprehensive review of FGA in the elderly. For this purpose, searches were done in PubMed, Medline, Web of Science, ScienceDirect, Cochrane Central Register of Controlled Clinical Trials, Google Scholar, Scopus, Magiran, Irandoc, IranMedex, MedLib, and SID databases from 1996 to November 2020.
Keywords
A search was performed in databases using the following keywords: 1) Walk; Gait; Locomot; Ambulat; AND 2) Elder; Old; Older adult; Senescent; Senile; Aged; Gray; Geriatric; Age; Aging; AND 3) Functional tests; Physical examination; Functional performance tests; Lower extremity tests. The “AND” operator was used between the 3 keyword groups, while the “OR” operator was used within each keyword group. After collecting the search results, first, the titles were studied followed by the abstracts. If an article matched the inclusion and exclusion criteria, its results were used in the review study; otherwise, it was excluded. Based on the criteria and objectives of the research, 19 articles were selected after evaluation. All articles were provided in full text.
Exclusion and inclusion criteria
Inclusion criteria: In the first stage, the titles and abstracts of descriptive studies were screened with a focus on FGA in the elderly and their publication in Persian and English. Then, a research assistant independently reviewed the abstracts of the articles. The second step involved screening the entire text by a researcher concerning the release of the index (i.e. FGA in the elderly) and a specific target population (i.e. elderly). A senior researcher then checked the final list of selected papers to ensure that all papers aligned with the research objectives. A summary of the descriptive information was then collected by the research assistant and checked by the senior researcher. A sample table (Figure 1) was used to extract information about the target population, FGA in the elderly, and their results.
Quality of evidence
The risk of bias was evaluated by both reviewers using Newcastle-Ottawa Quality Assessment Scale (NOS) [11]. Herzog et al.’s checklist for cross-sectional studies was employed [11]. Quality was assessed based on Herzog et al., as follows: Very Good Studies: 9-10 stars, Good Studies: 7-8 stars, Satisfactory Studies: 5-6 stars, Unsatisfactory Studies: 0-4 stars [11].
Data extraction
Data from studies were extracted independently by Researchers using some measures including the first reference and name of functional tests, validity, reliability, an explanation of how to evaluate and perform functional tests, and quality of evidence (Table 1).
Results
An electronic resource search yielded 367 titles. Furthermore, manually searching and reviewing the sources of articles gained 10 more titles. Following the removal of duplicate titles, 189 abstracts were identified for review. After reviewing the articles’ titles and abstracts, 145 articles were excluded, and 44 articles were selected to read the full text. After reviewing the articles’ full text, we selected and reported the results of 19 articles from 23 different tests, which studied FGA in the elderly (Table 1).
Based on the results of NOS, studies that were systematically reviewed had desirable qualities: 5 studies (22%) as very good (9-10 stars); 10 studies (44%) as good (7-8 stars), and 8 studies (34%) as satisfactory. Therefore, the studies that were systematically reviewed are of a very good to satisfactory quality. Results were shown in Table 1.
Discussion
This study aimed to evaluate FGA methods in the elderly. A review of the studies revealed that the studies used several methods to evaluate FGA in the elderly. In this review study, 19 articles were found from 23 multiple tests that attempted to examine FGA in the elderly. The features of these tests are discussed below.
An important factor examined in most FGAs in the elderly is gait assessment in the elderly speed [13, 21, 22, 26, 28]. Older people who take the test will score high in a short period, indicating that they are less prone to falls. Studies have examined the relationship between gait velocity and the risk of falling elderly [30, 31]. According to the results, the lower the gait speed in the elderly, the higher the risk of falls. Moreover, gait speed tests suitable for the elderly have been identified. Attempts have been made to answer the following questions: “Should tests be used in which the elderly are asked to walk at maximum speed or normal speed?” “Which of these factors best predicts the risk of falls in the elderly?” A study showed that both normal gait and gait factors with maximum speed could well predict the risk of falls in the elderly [32]. Therefore, in the case of gait in the elderly speed factor assessment tests, no distinction can be made between the tests that examined the maximum gait in the elderly rate and those that examined their normal gait rate. Both can predict the risk of falls in the elderly with approximately an equal probability.
Additionally, a 6-minute walking test [27] is designed to assess lower extremity muscle endurance in the elderly. In this test, the older the person who can walk, the more distance in 6 minutes and the higher the score, indicating a better physical condition of the elderly. Studies have evaluated the ability of the 6-minute walking test to predict the risk of falls in the elderly [33, 34]. The results showed that the 6-minute walking test could predict the risk of falls in the elderly with greater accuracy. It is also closely related to other physiological and psychological factors of the elderly. Therefore, it can be concluded that the 6-minute walking test is a practical test for assessing gait in the elderly. The results of this test can be used to evaluate the functional characteristics and risk of falls in the elderly.
Furthermore, among the FGA, several tests have examined gait by adding functional and cognitive tasks to the case [24, 25, 26, 27, 28, 29]. Several tasks were imposed on the elderly during gait to approximate the normal daily life of the elderly and to examine the elderly gait. These studies have shown that several other posture control factors may be involved in gait in the elderly and increase the risk of falls in the elderly. Therefore, these studies attempted to examine gait in the elderly by giving multiple tasks. Several studies have also investigated the effect of these tasks on gait in the elderly [35, 36, 37]. They concluded that multiple posture control factors could affect gait in the elderly, and consequently, increase the risk of falls in the elderly [38]. Studies have shown that the risk of falls in the elderly increases by adding task posture control during gait [39].
Therefore, it can be concluded that the purpose of designing these tests is to examine the effect of several different tasks during gait in the elderly. The results of this test can help accurately and correctly predict the physical condition and the risk of falls in the elderly.
Features of a valid functional test include validity, reliability, sensitivity, and high specificity. This review study examined FGA and found that validity and reliability were reported for most FGAs. However, few studies have addressed the sensitivity and specificity of FGA in the elderly. The sensitivity and specificity of tests were not reported for most FGAs. Sensitivity means that the number of people who fall is correctly identified, and specificity means that the number of people who do not fall is correctly identified. High sensitivity indicates that the test is suitable for screening.
On the other hand, high specificity indicates that the test is suitable for diagnosis. Therefore, studies should also specifically address the sensitivity and specificity of FGA in the elderly, as they help to more accurately analyze gait in the elderly functional tests. As a result, more accurate and appropriate interventions and programs can be developed following FGA measurements in the elderly.
This review study used a systematic search methodology but failed to quantify the articles. Although most articles taken from reputable international scientific-research journals are domestic and have an acceptable quality rating, care should be taken in generalizing their results. Moreover, although complete search strategies were used, only English and Persian articles were reviewed. There may be other related articles in other languages. Therefore, considering the mentioned limitations, future research should review the articles qualitatively.
Conclusion
Studies show that they treat FGA in the elderly using different methods and for different purposes. Studies to measure gait speed, normal gait, gait, and functional and cognitive tasks have helped measure functional gait in the elderly. Few studies have addressed the two main features of a valid test, sensitivity, and specificity. Studies should focus as much as possible on these test features in measuring FGA in the elderly.
Ethical Considerations
Compliance with ethical guidelines
Since this study is a review and does not require ethical approval, no university has been approved by the ethics committee. Also, the ethical principles in writing the article have been observed according to the instructions of the National Ethics Committee and the COPE regulations.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: All authors; Methodology and Investigation: Esmail Balaiy, Hamed Zarei; Supervision, Writing--original draft, Writing--review & editing: Ali Asghar Norasteh, Hamed Zarei; Funding acquisition: Esmail Balaiy; Resources: All author.
Conflict of interest
The authors report no conflict of interest.
Acknowledgements
The researchers thank the head of the Faculty of Physical Education, University of Guilan, Iran.
References
- Curcio F, Basile C, Liguori I, Della-Morte D, Gargiulo G, Galizia G, et al. Tinetti mobility test is related to muscle mass and strength in non-institutionalized elderly people. Age. 2016; 38(5-6):525-33. [DOI:10.1007/s11357-016-9935-9] [PMID] [PMCID]
- Gama ZA, Gómez-Conesa A. [Risk factors for falls in the elderly: Systematic review (Spanish)]. Rev Saude Publica. 2008; 42(5):946-56. [DOI:10.1590/S0034-89102008000500022] [PMID]
- Heinrich S, Rapp K, Rissmann U, Becker C, König HH. Cost of falls in old age: A systematic review. Osteoporos Int. 2010; 21(6):891-902. [DOI:10.1007/s00198-009-1100-1] [PMID]
- Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E. Risk factors for falls in community-dwelling older people: A systematic review and meta-analysis. Epidemiology. 2010; 21(5):658-68. [DOI:10.1097/EDE.0b013e3181e89905] [PMID]
- Gates S, Smith LA, Fisher JD, Lamb SE. Systematic review of accuracy of screening instruments for predicting fall risk among independently living older adults. J Rehabil Res Dev. 2008; 45(8):1105-16. [PMID]
- Dolatabadi E, Van Ooteghem K, Taati B, Iaboni A. Quantitative mobility assessment for fall risk prediction in dementia: A systematic review. Dement Geriatr Cogn Disord. 2018; 45(5-6):353-67.[DOI:10.1159/000490850] [PMID]
- Verghese J, Holtzer R, Lipton RB, Wang C. Quantitative gait markers and incident fall risk in older adults. J Gerontol A Biol Sci Med Sci. 2009; 64(8):896-901. [DOI:10.1093/gerona/glp033] [PMID] [PMCID]
- Hamacher D, Singh NB, Van Dieën JH, Heller MO, Taylor WR. Kinematic measures for assessing gait stability in elderly individuals: A systematic review. J R Soc Interface. 2011; 8(65):1682-98. [DOI:10.1098/rsif.2011.0416] [PMID] [PMCID]
- Kearney FC, Harwood RH, Gladman JR, Lincoln N, Masud T. The relationship between executive function and falls and gait abnormalities in older adults: A systematic review. Dement Geriatr Cogn Disord. 2013; 36(1-2):20-35. [DOI:10.1159/000350031] [PMID]
- Toebes MJ, Hoozemans MJ, Furrer R, Dekker J, van Dieën JH. Local dynamic stability and variability of gait are associated with fall history in elderly subjects. Gait Posture. 2012; 36(3):527-31. [DOI:10.1016/j.gaitpost.2012.05.016] [PMID]
- Herzog R, Álvarez-Pasquin MJ, Díaz C, Del Barrio JL, Estrada JM, Gil Á. Are healthcare workers' intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health. 2013; 13:154. [DOI:10.1186/1471-2458-13-154] [PMID] [PMCID]
- Botolfsen P, Helbostad JL, Moe-Nilssen R, Wall JC. Reliability and concurrent validity of the Expanded Timed Up-and-Go test in older people with impaired mobility. Physiother Res Int. 2008; 13(2):94-106. [DOI:10.1002/pri.394] [PMID]
- Peters DM, Fritz SL, Krotish DE. Assessing the reliability and validity of a shorter walk test compared with the 10-Meter Walk Test for measurements of gait speed in healthy, older adults. J Geriatr Phys Ther. 2013; 36(1):24-30.[DOI:10.1519/JPT.0b013e318248e20d] [PMID]
- Veronese N, Bolzetta F, Toffanello ED, Zambon S, De Rui M, Perissinotto E, et al. Association between Short Physical Performance Battery and falls in older people: The Progetto Veneto Anziani Study. Rejuvenation Res. 2014; 17(3):276-84. [DOI:10.1089/rej.2013.1491] [PMID] [PMCID]
- Rikli RE, Jones CJ. Development and validation of a functional fitness test for community-residing older adults. J Aging Phys Act. 1999; 7(2):129-61. [DOI:10.1123/japa.7.2.129]
- Hess RJ, Brach JS, Piva SR, VanSwearingen JM. Walking skill can be assessed in older adults: Validity of the Figure-of-8 Walk Test. Phys Ther. 2010; 90(1):89-99.[DOI:10.2522/ptj.20080121] [PMID] [PMCID]
- Latorre Román PÁ, Muñoz Jiménez M, Salas Sánchez J, Consuegra González P, Moreno Del Castillo R, et al. Complex gait is related to cognitive functioning in older people: A cross-sectional study providing an innovative test. Gerontology. 2020; 66(4):401-8. [DOI:10.1159/000508245] [PMID]
- Newell AM, VanSwearingen JM, Hile E, Brach JS. The modified Gait Efficacy Scale: establishing the psychometric properties in older adults. Phys Ther. 2012; 92(2):318-28.[DOI:10.2522/ptj.20110053] [PMID] [PMCID]
- Herman T, Inbar-Borovsky N, Brozgol M, Giladi N, Hausdorff JM. The dynamic gait index in healthy older adults: the role of stair climbing, fear of falling and gender. Gait Posture. 2009; 29(2):237-41. [DOI:10.1016/j.gaitpost.2008.08.013] [PMID] [PMCID]
- Chen S. Effect of Tai Chi exercises on the balance, functional gait, and flexibility of elderly Filipino males. Adv Soc Sci, Educ Humanit Res. 2019; 268:147-53. [DOI:10.2991/sohe-19.2019.25]
- Alfaro-Acha A, Al Snih S, Raji MA, Markides KS, Ottenbacher KJ. Does 8-foot walk time predict cognitive decline in older Mexicans Americans? J Am Geriatr Soc. 2007; 55(2):245-51 [DOI:10.1111/j.1532-5415.2007.01039.x] [PMID]
- Akbari Kamrani A A, Zamani Sani S H, Fathi Rezaie Z, Aghdasi M T. [Concurrent validity of functional gait assessment, timed up and go, and gait speed tests in the Persian community-dwelling elderly (Persian)]. Iran Rehab J. 2010; 8(2):15-20. [Link]
- Atkinson HH, Rosano C, Simonsick EM, Williamson JD, Davis C, Ambrosius WT, et al. Cognitive function, gait speed decline, and comorbidities: The health, aging and body composition study. J Gerontol A Biol Sci Med Sci. 2007; 62(8):844-50. [DOI:10.1093/gerona/62.8.844] [PMID]
- Watson NL, Rosano C, Boudreau RM, Simonsick EM, Ferrucci L, Sutton-Tyrrell K,et al. Executive function, memory, and gait speed decline in well-functioning older adults. J Gerontol A Biol Sci Med Sci. 201; 65(10):1093-100. [DOI:10.1093/gerona/glq111] [PMID] [PMCID]
- Lee HS, Park SW. The reliability of balance, gait, and muscle strength test for the elderly with dementia: A systematic review. J Korean Soc Phys Med. 2017; 12(3):49-58. [DOI:10.13066/kspm.2017.12.3.49]
- Sipilä S, Multanen J, Kallinen M, Era P, Suominen H. Effects of strength and endurance training on isometric muscle strength and walking speed in elderly women. Acta Physiol Scand. 1996; 156(4):457-64. [DOI:10.1046/j.1365-201X.1996.461177000.x] [PMID]
- Jenkins S, Cecins N, Camarri B, Williams C, Thompson P, Eastwood P. Regression equations to predict 6-minute walk distance in middle-aged and elderly adults. Physiother Theory Pract. 2009; 25(7):516-22. [DOI:10.3109/09593980802664711] [PMID]
- Cederberg KL, Motl RW, McAuley E. Physical activity, sedentary behavior, and physical function in older adults with Multiple Sclerosis. J Aging Phys Act. 2018; 26(2):177-82. [DOI:10.1123/japa.2016-0358] [PMID]
- Dyer AH, Lawlor B, Kennelly SP. Gait speed, cognition and falls in people living with mild-to-moderate Alzheimer disease: Data from NILVAD. BMC Geriatr. 2020; 20:117. [Link]
- Roos PE, Dingwell JB. Using dynamic walking models to identify factors that contribute to increased risk of falling in older adults. Hum Mov Sci. 2013; 32(5):984-96[DOI:10.1016/j.humov.2013.07.001] [PMID] [PMCID]
- Morita M, Takamura N, Kusano Y, Abe Y, Moji K, Takemoto T, et al. Relationship between falls and physical performance measures among community-dwelling elderly women in Japan. Aging Clin Exp Res. 2005; 17(3):211-6. [DOI:10.1007/BF03324599] [PMID]
- Middleton A, Fulk GD, Herter TM, Beets MW, Donley J, Fritz SL. Self-selected and maximal walking speeds provide greater insight into fall status than walking speed reserve among community-dwelling older adults. Am J Phys Med Rehabil. 2016; 95(7):475-82. [DOI:10.1097/PHM.0000000000000488] [PMID] [PMCID]
- Lord SR, Menz HB. Physiologic, psychologic, and health predictors of 6-minute walk performance in older people. Arch Phys Med Rehabil. 2002; 83(7):907-11. [DOI:10.1053/apmr.2002.33227] [PMID]
- Buisseret F, Catinus L, Grenard R, Jojczyk L, Fievez D, Barvaux V, et al. Timed up and go and six-minute walking tests with wearable inertial sensor: One step further for the prediction of the risk of fall in elderly nursing home people. Sensors (Basel). 2020; 20(11):3207. [DOI:10.3390/s20113207] [PMID] [PMCID]
- Montero-Odasso M, Verghese J, Beauchet O, Hausdorff JM. Gait and cognition: A complementary approach to understanding brain function and the risk of falling. J Am Geriatr Soc. 2012; 60(11):2127-36.[DOI:10.1111/j.1532-5415.2012.04209.x] [PMID] [PMCID]
- Segev-Jacubovski O, Herman T, Yogev-Seligmann G, Mirelman A, Giladi N, Hausdorff JM. The interplay between gait, falls and cognition: can cognitive therapy reduce fall risk? Expert Rev Neurother. 2011; 11(7):1057-75. [DOI:10.1586/ern.11.69] [PMID] [PMCID]
- St George RJ, Fitzpatrick RC, Rogers MW, Lord SR. Choice stepping response and transfer times: effects of age, fall risk, and secondary tasks. J Gerontol A Biol Sci Med Sci. 2007; 62(5):537-42. [DOI:10.1093/gerona/62.5.537] [PMID]
- Ambrose AF, Paul G, Hausdorff JM. Risk factors for falls among older adults: A review of the literature. Maturitas. 2013; 75(1):51-61. [DOI:10.1016/j.maturitas.2013.02.009] [PMID]
- Al-Yahya E, Dawes H, Smith L, Dennis A, Howells K, Cockburn J. Cognitive motor interference while walking: A systematic review and meta-analysis. Neurosci Biobehav Rev. 2011; 35(3):715-28. [DOI:10.1016/j.neubiorev.2010.08.008] [PMID]
Type of Study: Review |
Subject:
Special
Received: 2022/12/19 | Accepted: 2020/04/22 | Published: 2023/04/23
Received: 2022/12/19 | Accepted: 2020/04/22 | Published: 2023/04/23
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
