Mon, May 6, 2024
Volume 5, Issue 1 (Winter 2019)
Caspian J Neurol Sci 2019, 5(1): 7-15 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rezaei S, Mahfeli M, Mousavi S V, Poorabolghasem Hosseini S. The Effect of Laughter Yoga on the Quality of Life of Elderly Nursing Home Residents. Caspian J Neurol Sci 2019; 5 (1) :7-15
URL: http://cjns.gums.ac.ir/article-1-254-en.html
URL: http://cjns.gums.ac.ir/article-1-254-en.html



1- Department of Psychology, Faculty of Literature and Humanities, University of Guilan, Rasht, Iran , rezaei_psy@hotmail.com
2- Department of Psychology, Faculty of Literature and Humanities, University of Guilan, Rasht, Iran
2- Department of Psychology, Faculty of Literature and Humanities, University of Guilan, Rasht, Iran
Full-Text [PDF 1567 kb]
(1663 Downloads)
| Abstract (HTML) (3327 Views)
Full-Text: (1475 Views)
Introduction
Reports suggest that, by 2030, the world’s aging population will increase from 9% to 16% and in Iran from 5.6% to 17.5%. With the rise of the aging population, attention to their problems becomes more important in the world and Iran and calls for research in this area [1]. The old age is a period of life that begins at age 60 and is a biological process that all living beings, including humans, experience it [2]. This period, with all of its consequences for the individuals and society, has created major challenges for all communities [3]. The elderly people are at risk of potential threats, such as increased chronic diseases, loneliness, isolation, and lack of social support [4].
The old age is significantly associated with adverse health outcomes, such as physical comorbidities, poor mental health, and damaged cognitive function, which lowers quality of life [5]. Psychological disorders such as depression and anxiety affect the quality of life of the elderly [6, 7]. Quality of Life (QoL) is defined as people’s perception of their position in life and in relation to their goals in the context of culture and value systems in which they live. QoL includes physical health, psychological state, social relationships, and environmental factors. The combined effects of economic, political and social stress affect the QoL of a person [8]. Occupational stresses and the complexities of modern life have caused family members miss the time and energy to care for the elderly. Hence they keep them in nursing homes. As a result of this detachment from the family, the older people’s mental health, happiness, and satisfaction with life are affected [4].
Laughter is a universal sign of happiness. Laughter is at the center of research attention for two reasons: a. It can increase mood, optimism, energy, and cognitive function; and b. It can reduce anxiety, stress, loneliness, depression, and tension [9]. Laughter Therapy (LT) has a long history. The scientific study of laughter began by Dr. William Fry at Stanford University in 1964. He pointed to the importance of humor and laughter in aging and argued the benefits of laughter on blood pressure and cardiovascular system [9]. There is an LT technique that mixes unconditional laughter and yoga breathing exercises which was popularized by Madan Kataria. In this technique called “Laughter Yoga”, laughing exercises are combined with yoga exercises. In one session, faking laughter is produced through physical exercises, interacting with other group members, and playing children’s games. In most cases, fake laughter infects other members, because people cannot distinguish between fake and real laughter [10].
Low mobility, low physical activity and lack of motivation for regular physical activity are common problems that have negative effects on the QoL of the elderly people [11]. On the other hand, high levels of physical activity are associated with better QoL, longer lifespan, and better cognitive function [12, 13]. Therefore, considering the physical constraints of the elderly living in nursing homes, it is thought that the use of joyful interventions such as LT can help improve their QoL [14]. Gonot-Schoupinsky and Garip in a systematic review reported the benefits of laughter and humor on well-being which include improvement of the circulatory system, musculoskeletal system, digestive system, respiratory system as well as the regulation of hormones, sleep and resting cycles, and strengthening of the immune system [9]. They argued that laughter interventions with humor are effective in increasing the well-being of the elderly. Lebowitz et al. showed that laughter in patients with pulmonary disease can reduce their depression and anxiety and improve their QoL [15].
Kuru and Kublay suggested that nurses of nursing homes should use LT as an intervention for improving the QoL of the residents [14]. They found out that LT had a positive effect on the QoL of older people in Turkey. Ko and Youn believed that LT was useful, accessible, and economically affordable [16]. They reported that laughter interventions have positive effects on improving depression and insomnia and promoting QoL. However, Cho and Oh in a study on patients with breast cancer, found out that LT cannot improve the depression and immune response of these patients, but can improve their QoL and resilience [17].
In Iran, Ghodsbin et al. concluded that LT can improve the general health of the elderly people referring to Shiraz elderly people club [18]. In addition, Bayat et al. showed that LT and physical activity can reduce the feeling of loneliness and increase the happiness of older people [19]. However, there is not enough evidence that LT with a variety of other intervening factors, can increase well-being. There are considerable studies on the effects of LT on physical and mental issues [14-19], but less information was found about the effect of this therapy on the residents of nursing homes, especially in Iran. Therefore interventions based on the laughter are important for the older population. This study was conducted to evaluate the effect of Laughter Therapy on the QoL of elderly people and investigating two hypotheses: 1. LT affects the QoL of elderly people; and 2. Its effects are still effective on the QoL of the elderly after one month follow-up period.
Materials and Methods
This is a quasi-experimental study with pre-test, post-test and follow-up design. The study population consisted of all elderly people living in nursing homes in Astaneh-ye Ashrafiyeh City, Iran. The samples were residents of Mehr Aein nursing home (n=44) in 2017. Out of them, 32 people were passed the General Health Questionnaire (28 items). The results indicated that all of them scored higher than 41 cut-off point, indicating their need for mental intervention. Then the sample was assigned to the experimental (LT group) and control groups. The demographic variables of the participants were as follows: their mean age; 72 years, 16 men and 16 women, 19 were illiterate, 3 had an elementary education, 4 passed guidance school, 2 had a diploma, 2 had Quranic literacy, 1 passed literacy movement program, and 1 was a physician.
The inclusion criteria were being older than 65 years and living in the nursing home, lacking severe and chronic physical and psychological illness according to medical records, obtaining a score >41 in General Health Questionnaire (GHQ-28), giving consent to participate in the study; not having dementia or severe disability, being able to verbally communicate with researchers, lacking hearing and speech impairment (after using hearing aids and glasses). The exclusion criteria were being too old to participate in the intervention, having severe memory loss, and unwillingness to continue the study.
Study tools
The 28-item General Health Questionnaire
To group the participants into the control and experimental, we used the 28-item General Health Questionnaire (GHQ-28). GHQ-28 was designed by Goldberg and Hiller in 1979 and have 4 subscales of somatic symptoms (items 1-7), anxiety/insomnia signs (items 8-14), social dysfunction (items 15-21), and depression (items 22-28). The items are rated based on a 4-point Likert-type scale from 0 to 3 [20]. Several studies have shown the questionnaire high validity and reliability for the Iranian elderly population. For example, Malakooti et al. reported the Cronbach alpha coefficient of 0.94 for its total scales and the mean correlation of items as 0.35 [21]. Also, they reported the Cronbach alpha coefficients of 0.89 for depression, 0.89 for social dysfunction, 0.85 for anxiety/insomnia, and 0.71 for somatic symptoms subscales [21]. In the present study, the internal consistency of this tool was obtained by Cronbach alpha as 0.67.
The elderly quality of life questionnaire
The elderly quality of life questionnaire (LIPAD) was used to assess QoL of subjects. It was designed by De Leo et al. in 1998 and used in three cities of Leiden in the Netherlands, Padua in Italy, and Helsinki in Finland [22]. This questionnaire has been translated in Iran and standardized. Its first part surveys personal and demographic characteristics and the second part consists of 31 items which assess 7 dimensions of QoL, including physical functioning (5 items), depression/anxiety (18 items), life satisfaction (6 items), and sexual functioning (2 items). Its rating is based on a 4-point Likert-type scale ranged from 0 to 3. In the study of Sajjadi and Biglareen, the reliability of this questionnaire was reported as 0.87 through calculation of the Cronbach alpha coefficient [23]. Its content validity also was reported acceptable by the experts.
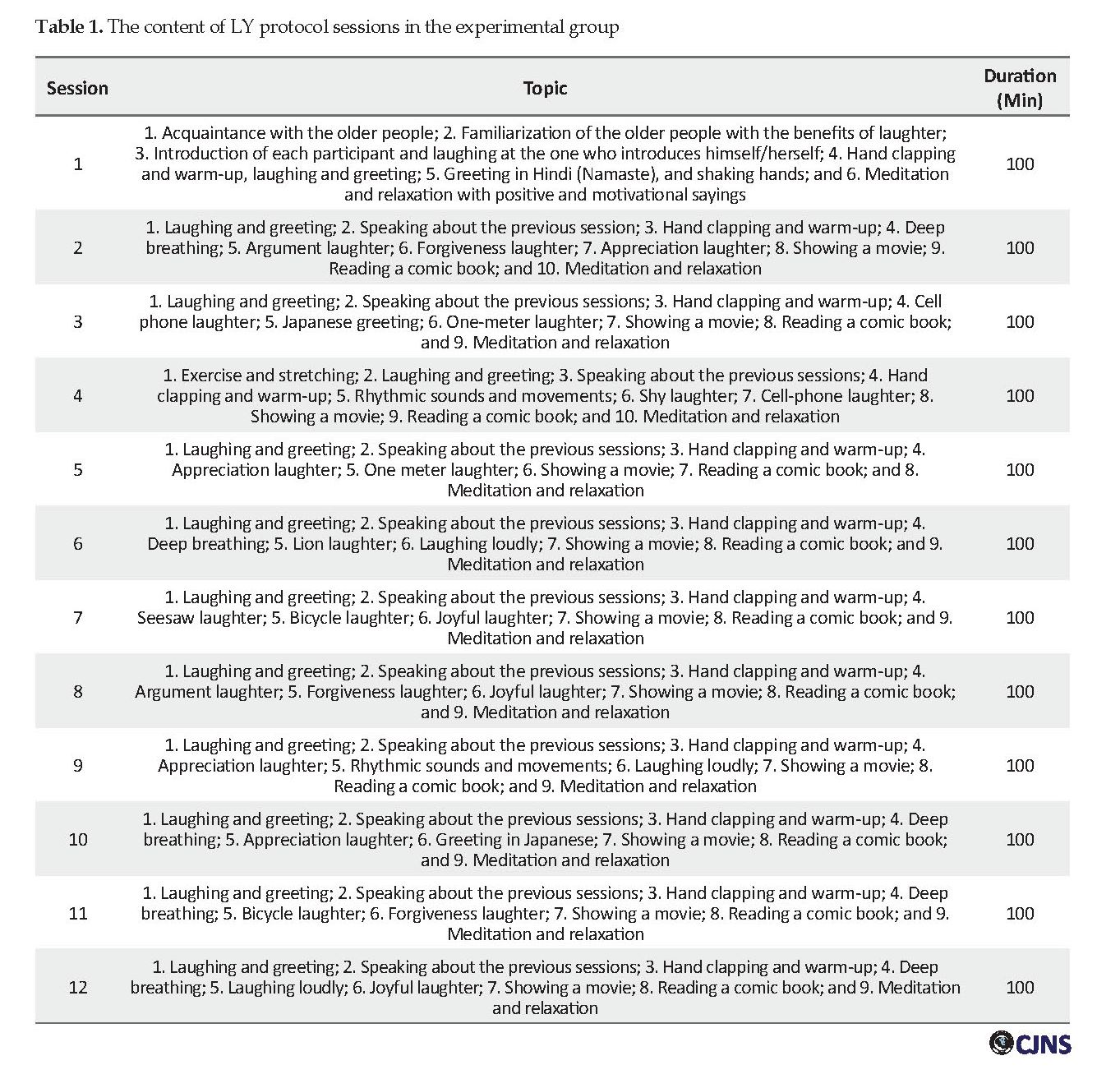
After the initial examination, it was found that 3 elderlies had severe disabilities, 4 had dementia and 5 were too old to communicate properly. Therefore, they were excluded from the study. Then the GHQ-28 was administered to 32 remaining subjects to determine their mental health based on 41 cut-off point [24]. Scores higher than 41 indicate the person’s need for psychological intervention. Before the intervention, both groups completed LIPAD questionnaire. Then, the experimental group received Laughter Yoga (LY) according to Madan Kataria method (twelve 100-minute sessions) which has been summarized in Table 1 [10]. The control group received no intervention.
The intervention package included LY, comic films, and books. LY consisted of 12 sessions for 100 minutes (3 sessions each week on Monday, Tuesday, and Thursday). Each session was a combination of stimulating laughs, breathing exercises, stretching movements, showing comic films and reading comic books. After completing the intervention, both groups again completed LIPAD questionnaire. After one month, the above test was performed again (1-month follow-up). The obtained data were analyzed with descriptive statistics (mean and standard deviation) and 1-way ANCOVA in the form of a 3×2 design with repeated measurement. For considering ethical guidelines, the purpose of the study was explained to the participants and they were assured of the confidentiality of their information.
Results
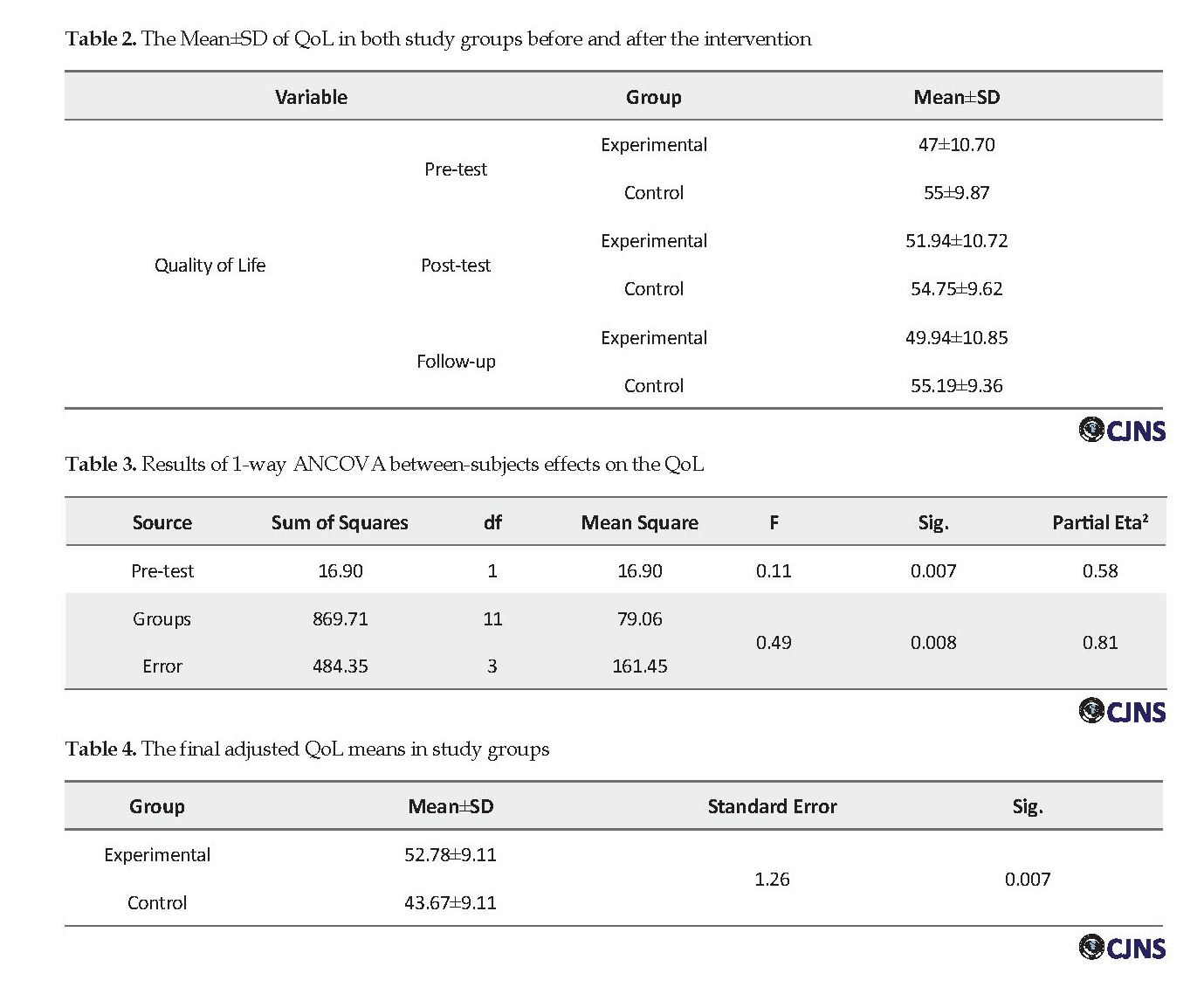
The study participants were 32 old people residing in Mehr Aein nursing home of Astaneh-ye Ashrafiyeh City with the mean age of 71 years for the experimental (LT group) group, and 73 years for the control group. Table 2 presents descriptive statistics (Mean±SD) of QoL in subjects before and after LY intervention.
According to the results, the mean post-test QoL score of the experimental group was lower than that of the control group. In the follow-up period, QoL score in the experimental group was also less than that in the control group. Since the experimental group was very different from the control group in terms of the measured QoL indices, to reevaluate and revise the improvement of this group indices in response to Laughter Therapy, their adjusted mean scores should be evaluated. Although in terms of General Health Questionnaire (GHQ-28), they were equal (P>0.05), the QoL scores of the subjects were considerably different after grouping them into the experimental and control. However, pre-test scores of both groups were considered as covariates.
Reports suggest that, by 2030, the world’s aging population will increase from 9% to 16% and in Iran from 5.6% to 17.5%. With the rise of the aging population, attention to their problems becomes more important in the world and Iran and calls for research in this area [1]. The old age is a period of life that begins at age 60 and is a biological process that all living beings, including humans, experience it [2]. This period, with all of its consequences for the individuals and society, has created major challenges for all communities [3]. The elderly people are at risk of potential threats, such as increased chronic diseases, loneliness, isolation, and lack of social support [4].
The old age is significantly associated with adverse health outcomes, such as physical comorbidities, poor mental health, and damaged cognitive function, which lowers quality of life [5]. Psychological disorders such as depression and anxiety affect the quality of life of the elderly [6, 7]. Quality of Life (QoL) is defined as people’s perception of their position in life and in relation to their goals in the context of culture and value systems in which they live. QoL includes physical health, psychological state, social relationships, and environmental factors. The combined effects of economic, political and social stress affect the QoL of a person [8]. Occupational stresses and the complexities of modern life have caused family members miss the time and energy to care for the elderly. Hence they keep them in nursing homes. As a result of this detachment from the family, the older people’s mental health, happiness, and satisfaction with life are affected [4].
Laughter is a universal sign of happiness. Laughter is at the center of research attention for two reasons: a. It can increase mood, optimism, energy, and cognitive function; and b. It can reduce anxiety, stress, loneliness, depression, and tension [9]. Laughter Therapy (LT) has a long history. The scientific study of laughter began by Dr. William Fry at Stanford University in 1964. He pointed to the importance of humor and laughter in aging and argued the benefits of laughter on blood pressure and cardiovascular system [9]. There is an LT technique that mixes unconditional laughter and yoga breathing exercises which was popularized by Madan Kataria. In this technique called “Laughter Yoga”, laughing exercises are combined with yoga exercises. In one session, faking laughter is produced through physical exercises, interacting with other group members, and playing children’s games. In most cases, fake laughter infects other members, because people cannot distinguish between fake and real laughter [10].
Low mobility, low physical activity and lack of motivation for regular physical activity are common problems that have negative effects on the QoL of the elderly people [11]. On the other hand, high levels of physical activity are associated with better QoL, longer lifespan, and better cognitive function [12, 13]. Therefore, considering the physical constraints of the elderly living in nursing homes, it is thought that the use of joyful interventions such as LT can help improve their QoL [14]. Gonot-Schoupinsky and Garip in a systematic review reported the benefits of laughter and humor on well-being which include improvement of the circulatory system, musculoskeletal system, digestive system, respiratory system as well as the regulation of hormones, sleep and resting cycles, and strengthening of the immune system [9]. They argued that laughter interventions with humor are effective in increasing the well-being of the elderly. Lebowitz et al. showed that laughter in patients with pulmonary disease can reduce their depression and anxiety and improve their QoL [15].
Kuru and Kublay suggested that nurses of nursing homes should use LT as an intervention for improving the QoL of the residents [14]. They found out that LT had a positive effect on the QoL of older people in Turkey. Ko and Youn believed that LT was useful, accessible, and economically affordable [16]. They reported that laughter interventions have positive effects on improving depression and insomnia and promoting QoL. However, Cho and Oh in a study on patients with breast cancer, found out that LT cannot improve the depression and immune response of these patients, but can improve their QoL and resilience [17].
In Iran, Ghodsbin et al. concluded that LT can improve the general health of the elderly people referring to Shiraz elderly people club [18]. In addition, Bayat et al. showed that LT and physical activity can reduce the feeling of loneliness and increase the happiness of older people [19]. However, there is not enough evidence that LT with a variety of other intervening factors, can increase well-being. There are considerable studies on the effects of LT on physical and mental issues [14-19], but less information was found about the effect of this therapy on the residents of nursing homes, especially in Iran. Therefore interventions based on the laughter are important for the older population. This study was conducted to evaluate the effect of Laughter Therapy on the QoL of elderly people and investigating two hypotheses: 1. LT affects the QoL of elderly people; and 2. Its effects are still effective on the QoL of the elderly after one month follow-up period.
Materials and Methods
This is a quasi-experimental study with pre-test, post-test and follow-up design. The study population consisted of all elderly people living in nursing homes in Astaneh-ye Ashrafiyeh City, Iran. The samples were residents of Mehr Aein nursing home (n=44) in 2017. Out of them, 32 people were passed the General Health Questionnaire (28 items). The results indicated that all of them scored higher than 41 cut-off point, indicating their need for mental intervention. Then the sample was assigned to the experimental (LT group) and control groups. The demographic variables of the participants were as follows: their mean age; 72 years, 16 men and 16 women, 19 were illiterate, 3 had an elementary education, 4 passed guidance school, 2 had a diploma, 2 had Quranic literacy, 1 passed literacy movement program, and 1 was a physician.
The inclusion criteria were being older than 65 years and living in the nursing home, lacking severe and chronic physical and psychological illness according to medical records, obtaining a score >41 in General Health Questionnaire (GHQ-28), giving consent to participate in the study; not having dementia or severe disability, being able to verbally communicate with researchers, lacking hearing and speech impairment (after using hearing aids and glasses). The exclusion criteria were being too old to participate in the intervention, having severe memory loss, and unwillingness to continue the study.
Study tools
The 28-item General Health Questionnaire
To group the participants into the control and experimental, we used the 28-item General Health Questionnaire (GHQ-28). GHQ-28 was designed by Goldberg and Hiller in 1979 and have 4 subscales of somatic symptoms (items 1-7), anxiety/insomnia signs (items 8-14), social dysfunction (items 15-21), and depression (items 22-28). The items are rated based on a 4-point Likert-type scale from 0 to 3 [20]. Several studies have shown the questionnaire high validity and reliability for the Iranian elderly population. For example, Malakooti et al. reported the Cronbach alpha coefficient of 0.94 for its total scales and the mean correlation of items as 0.35 [21]. Also, they reported the Cronbach alpha coefficients of 0.89 for depression, 0.89 for social dysfunction, 0.85 for anxiety/insomnia, and 0.71 for somatic symptoms subscales [21]. In the present study, the internal consistency of this tool was obtained by Cronbach alpha as 0.67.
The elderly quality of life questionnaire
The elderly quality of life questionnaire (LIPAD) was used to assess QoL of subjects. It was designed by De Leo et al. in 1998 and used in three cities of Leiden in the Netherlands, Padua in Italy, and Helsinki in Finland [22]. This questionnaire has been translated in Iran and standardized. Its first part surveys personal and demographic characteristics and the second part consists of 31 items which assess 7 dimensions of QoL, including physical functioning (5 items), depression/anxiety (18 items), life satisfaction (6 items), and sexual functioning (2 items). Its rating is based on a 4-point Likert-type scale ranged from 0 to 3. In the study of Sajjadi and Biglareen, the reliability of this questionnaire was reported as 0.87 through calculation of the Cronbach alpha coefficient [23]. Its content validity also was reported acceptable by the experts.
After the initial examination, it was found that 3 elderlies had severe disabilities, 4 had dementia and 5 were too old to communicate properly. Therefore, they were excluded from the study. Then the GHQ-28 was administered to 32 remaining subjects to determine their mental health based on 41 cut-off point [24]. Scores higher than 41 indicate the person’s need for psychological intervention. Before the intervention, both groups completed LIPAD questionnaire. Then, the experimental group received Laughter Yoga (LY) according to Madan Kataria method (twelve 100-minute sessions) which has been summarized in Table 1 [10]. The control group received no intervention.
The intervention package included LY, comic films, and books. LY consisted of 12 sessions for 100 minutes (3 sessions each week on Monday, Tuesday, and Thursday). Each session was a combination of stimulating laughs, breathing exercises, stretching movements, showing comic films and reading comic books. After completing the intervention, both groups again completed LIPAD questionnaire. After one month, the above test was performed again (1-month follow-up). The obtained data were analyzed with descriptive statistics (mean and standard deviation) and 1-way ANCOVA in the form of a 3×2 design with repeated measurement. For considering ethical guidelines, the purpose of the study was explained to the participants and they were assured of the confidentiality of their information.
Results
The study participants were 32 old people residing in Mehr Aein nursing home of Astaneh-ye Ashrafiyeh City with the mean age of 71 years for the experimental (LT group) group, and 73 years for the control group. Table 2 presents descriptive statistics (Mean±SD) of QoL in subjects before and after LY intervention.
According to the results, the mean post-test QoL score of the experimental group was lower than that of the control group. In the follow-up period, QoL score in the experimental group was also less than that in the control group. Since the experimental group was very different from the control group in terms of the measured QoL indices, to reevaluate and revise the improvement of this group indices in response to Laughter Therapy, their adjusted mean scores should be evaluated. Although in terms of General Health Questionnaire (GHQ-28), they were equal (P>0.05), the QoL scores of the subjects were considerably different after grouping them into the experimental and control. However, pre-test scores of both groups were considered as covariates.
After confirming the assumptions of covariance analysis, including the normal distribution of the variables, existence of a linear relationship between pre-test and post-test variables, homogeneity of errors variance, homogeneity of groups in variables pre-test, and equality of regression line slopes of variables in the pre-test and post-test in two groups, 1-way ANCOVA was used to evaluate the effect of LT on QoL of the elderly subjects.
According to Table 3, the F statistic of QoL is 0.49 in the post-test (P<0.01). This indicates a significant difference between the two groups in terms of QoL. Before the intervention, the F value was 0.11 (P<0.01), i.e. pre-test scores had a significant effect on the post-test scores and using ANCOVA is necessary. After controlling pre-test scores, to determine which of the groups had higher post-test QoL scores, adjusted means were calculated and reported (Table 4).
According to Table 3, the F statistic of QoL is 0.49 in the post-test (P<0.01). This indicates a significant difference between the two groups in terms of QoL. Before the intervention, the F value was 0.11 (P<0.01), i.e. pre-test scores had a significant effect on the post-test scores and using ANCOVA is necessary. After controlling pre-test scores, to determine which of the groups had higher post-test QoL scores, adjusted means were calculated and reported (Table 4).
According to Table 4, the mean QoL of the experimental group was 52.78 and for the control group 43.67. The mean difference between groups was 9.11 which was significant (P<0.01). Therefore, it can be said that the mean QoL of the experimental group was significantly higher than that of the control group. So our first hypothesis is confirmed which says “LT affects the QoL of the elderly people”.
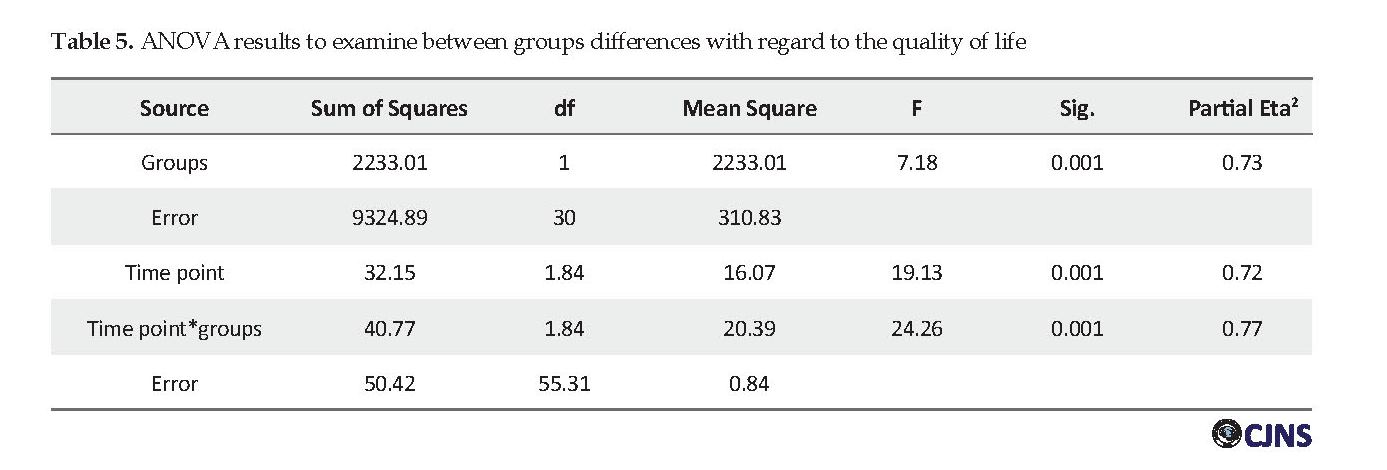
For assessing our second hypothesis which says “LT after one-month follow-up period continues to affect the QoL of the elderly,” by considering Huynh-Feldt correction (due to the significance of Mauchly’s test statistic and Epsilon value >0.75), repeated measures ANOVA was used which assessed the difference between samples in three time points of pre-test, post-test, and 1-month follow-up. The results are presented in Table 5.
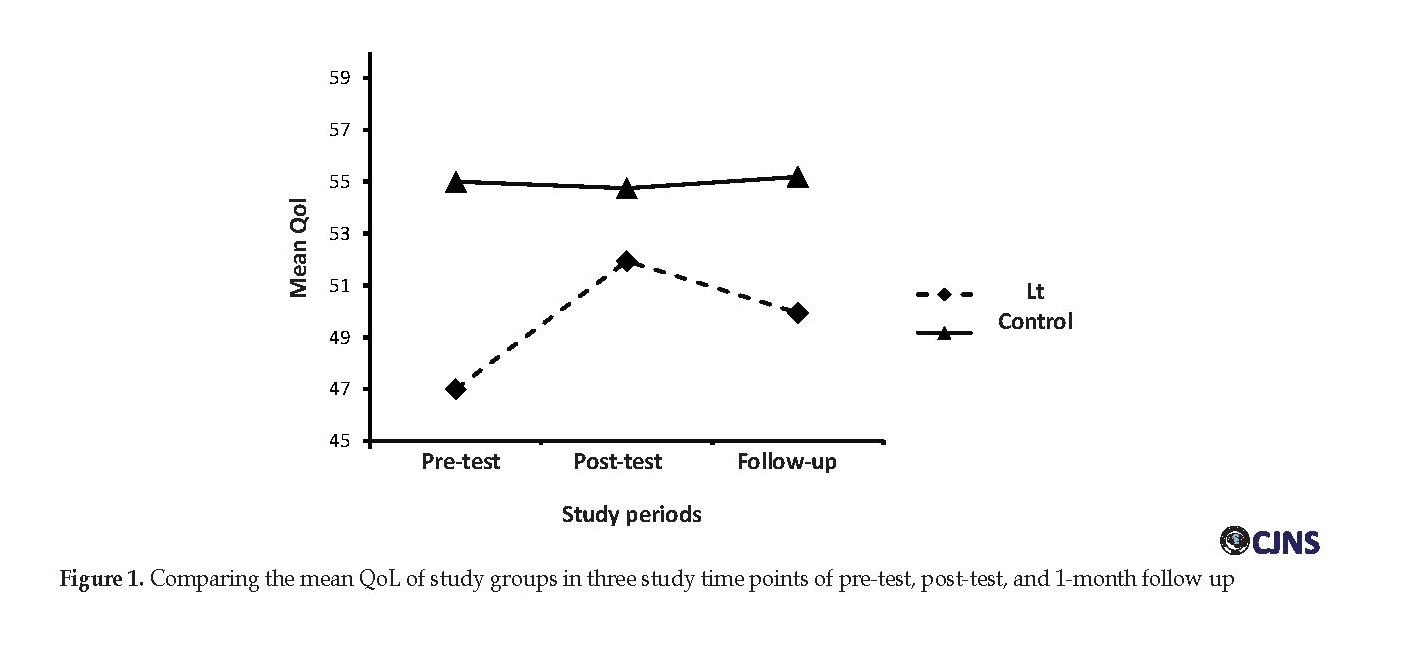
As seen in Table 5, F calculated value for the effect of the groups was 7.18 (P<0.01). Thus, there is a significant difference between the experimental and the control group. Also, the calculated F value for the time points was 19.13 (P<0.01). Hence, there is a significant difference between study time points. In addition, F=24.26 for the interaction between groups and periods (P<0.01). Thus, QoL changes in two groups of the experimental and control in three time points of pre-test, post-test, and 1-month follow-up are significantly different. Figure 1 illustrates these changes in the QoL of the groups in three time points.
As seen in Table 5, F calculated value for the effect of the groups was 7.18 (P<0.01). Thus, there is a significant difference between the experimental and the control group. Also, the calculated F value for the time points was 19.13 (P<0.01). Hence, there is a significant difference between study time points. In addition, F=24.26 for the interaction between groups and periods (P<0.01). Thus, QoL changes in two groups of the experimental and control in three time points of pre-test, post-test, and 1-month follow-up are significantly different. Figure 1 illustrates these changes in the QoL of the groups in three time points.
As can be observed, the mean post-test QoL score of the experimental group (51.94) is higher than that in the pre-test (47). Also in the follow-up period, the mean QoL score of the experimental group (49.94) is higher than that in the pre-test (47) which indicates the stability of treatment after one month. Overall, the mean QoL of the experimental group was lower than that of the control group in the pre-test, post-test and 1-month follow-up, because after the grouping of the subjects and from the beginning of the study, the control group had a better quality of life scores than the experimental group (although their GHQ-28 scores were equal). Hence, it can be said that LT (considering the baseline of the experimental group) had a positive effect on the QoL of those in the experimental group and helped them get closer to the scores of the elderlies in control group that were in a better situation. The comparison of the lines of each group in Figure 1 shows that in the experimental group from the pre-test to the post-test stage, an increase has occurred indicating a positive effect and QoL improvement. However, no increase was observed in the control group.
Discussion
This study was conducted with the aim of evaluating the effect of Laughter Therapy on QoL of the elderlies living in Astaneh-ye Ashrafiyeh nursing home. Our study results revealed a significant and positive effect of LT on the QoL of subjects. Also, a significant difference was observed between those in the LT group and the control group in terms of QoL. This finding is consistent with the findings of previous studies [14, 15, 17]. Hence, it can be said that LT which included a series of stimulated laughers, breathing and stretching exercises, watching films and reading comic books, influences the QoL of the elderlies in all aspects of physical functioning, depression/anxiety, life satisfaction, and sexual functioning.
Laughter increases the oxygenation of the body cells, strengthens the immune system, increases blood circulation, and creates positive mental health [25]. Different activities of the body such as deep breathing and intense muscle contractions caused by laughter, improve the contraction of the muscles and movement of the respiratory muscles [26]. Heo et al. on studying the effect of laughter on mood, cortisol levels, and QoL, revealed that LT, breathing, stretching exercises, and meditation had a positive effect on cortisol level and mood [27]. Thus, laughter with creating psychological and physiological changes can improve the QoL of the elderly.
Laughing is also a kind of meditation or relaxation. When people laugh, there is no thought in their minds. All the senses of the person are synchronized for the present moment without any effort and then, he or she feels joy, peace, and comfort [25]. Laughter as a psycho-physiological response to humor or any other similar stimuli such as positive feelings or pleasant thoughts is an activity that encourages the individual and leads to personal well-being. It also creates a positive feeling in the person that improves the way of thinking and QoL [28]. Results of Ko and Youn also indicated the positive effect of this intervention [16]. According to Kim et al. study, LT could also considerably reduce depression, anxiety, and stress [29].
Results of the current study also showed that after one month follow up, the LT program was effective in improving the QoL of the elderly people. In explaining this finding, it can be said that the effects of LT program on improving the QoL of elderly people was sustainable and effective. In this regard, a joyful program, movie, humor, and breathing exercises can sustainability reduce depression and anxiety, and increase the level of life satisfaction and physical well-being. Overall, to explain these findings, it can be said that LT as an intervention that combines relaxation, stretching movements, breathing exercise, joking and laughs, reduces depression, anxiety, and stress and increases hope in the elderly [29-31].
In other words, laughter as a coping mechanism is associated with increased self-efficacy and self-esteem and affects mood and depression. It influences hypothalamic-pituitary-adrenal axis via the central nervous system leading to a decrease in cortisol level and thus, a reduction in stress [32]. Moreover, laughter with stimulation of endorphin production increases the toleration to physical pain, and with increasing the contraction of facial muscles, blood flow, and adrenaline release in the blood increase happiness and joy [33]. The desirable outcome in such situation will be an improvement in QoL.
The results of this study indicate the effectiveness of Laughter Therapy on the quality of life of older people. To achieve more accurate results, it is recommended that future studies be conducted on the older people who do not live in nursing homes. Also, the effectiveness of the LT program can be investigated among the elderly with physical illnesses and their attitudes towards death and themselves. It should be noted that the present study had some limitations. For example, the study population was limited to one nursing home and some subjects were unable to complete the questionnaire due to their senility and low literacy level.
Conclusion
Considering the effectiveness of Laughter Therapy, it is possible to improve the quality of life of the elderly by applying this program. Hence, it is suggested that this program is used in the elderly nursing homes. Furthermore, due to the safety of this program and lack of any adverse effects on the elderly, authorities should consider the Laughter Therapy program as a complementary therapeutic approach along with other therapies to improve the quality of life of the elderly.
Ethical Considerations
Compliance with ethical guidelines
For considering ethical guidelines, the purpose of the study was explained to the participants and they were assured of the confidentiality of their information. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.For considering ethical guidelines, the purpose of the study was explained to the participants and they were assured of the confidentiality of their information.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
Draft: Shima Poorabolghasem Hosseini; Writing–review & editing: Sajjad Rezaei; Resources: All authors; Supervision: Seyed Valiollah Mousavi; and data collecting: Maryana Mahfeli.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
We appreciate the principal of Mehr Aein Nursing Home in Astaneh-ye Ashrafiyeh City (Northern Iran).
References
Khezri Moghadam N, Vahidi S, Ashormahani M. Efficiency of cognitive-existential group therapy on life expectancy and depression of elderly residing in nursing homes. Ageing. 2018; 13(1):62-73. [DOI:10.21859/sija.13.1.62]
Moatamedy A, Borjali A, Sadeqpur M. Prediction of psychological well-being of the elderly based on the power of stress management and social support. Ageing. 2018; 13(1):98-109. [DOI:10.21859/sija.13.1.98]
Mendoza-Nú-ez VM, Sarmiento-Salmorán E, Cortés RC, Maldonado MM, Ruiz-Ramos M. Influence of the self-perception of old age on the effect of a healthy aging program. J Clin Med. 2018; 7(106):1-11.
Saffarinia M, Dortaj A. Effect of group logotherapy on life expectancy and mental and social wellbeing of the female elderly residents of nursing homes in Dubai. Ageing. 2018; 12(4):482-93. [DOI:10.21859/sija.12.4.482]
Kuok K, Li L, Xiang YT, Nogueira BOCL, Ungvari GS, Ng CH, et al. Quality of Life and clinical correlates in older adults living in the community and in nursing homes in Macao. Psychogeriatr. 2017; 17(3):194-9. [DOI:10.1111/psyg.12214]
Canuto A, Weber K, Baertschi M, Andreas S, Volkert J, Dehoust MC, et al. Anxiety disorders in old age: psychiatric comorbidities, quality of life, and prevalence according to age, gender, and country. Am J Geriatr Psychiatry. 2018; 26(2):174-85. [DOI:10.1016/j.jagp.2017.08.015]
Becker NB, Jesus SN, Viseu JN, Stobäus CD, Guerreiro M, Domingues RB. Depression and quality of life in older adults: Mediation effect of sleep quality. Int J Clin Health Psychol. 2018; 18(1):8-17. [DOI:10.1016/j.ijchp.2017.10.002] [PMID] [PMCID]
World Health Organization. WHOQOL: Measuring Quality of Life. Geneva: World Health Organization; 2017.
Gonot-Schoupinsky FN, Garip G. Laughter and humour interventions for well-being in older adults: A systematic review and intervention classification. Complement Ther Med. 2018; 38:85-91. [DOI:10.1016/j.ctim.2018.04.009] [PMID]
Kataria M. Laugh for no reason. Mumbai: Madhuri International; 2005.
Schutzer KA, Graves BS. Barriers and motivations to exercise in older adults. Prev Med. 2004; 39(5):1056-61. [DOI:10.1016/j.ypmed.2004.04.003] [PMID]
Yen HY, Lin LJ. Quality of life in older adults: Benefits from the productive engagement in physical activity. J Exerc Sci Fit. 2018; 16(2):49-54. [DOI:10.1016/j.jesf.2018.06.001] [PMID] [PMCID]
Rezaei S, Montazar E, Mousavi SV, Poorabolghasem Hosseini Sh. Physical Activity and Cognitive Function in the Elderly Population. Caspian J Neurol Sci. 2018; 4(3):121-7.
Kuru N, Kublay G. The effect of Laughter Therapy on the quality of life of nursing home residents. J Clin Nurs. 2017; 26(21-22):3354-62. [DOI:10.1111/jocn.13687] [PMID]
Lebowitz KR, Suh S, Diaz PT, Emery CF. Effects of humor and laughter on psychological functioning, Quality of Life, health status, and pulmonary functioning among patients with chronic obstructive pulmonary disease: A preliminary investigation. Heart Lung. 2011; 40(4):310-9. [DOI:10.1016/j.hrtlng.2010.07.010] [PMID]
Ko HJ, Youn CH. Effects of Laughter Therapy on depression, cognition and sleep among the community‐dwelling elderly. Geriatr Gerontol Int. 2011; 11(3):267-74. [DOI:10.1111/j.1447-0594.2010.00680.x] [PMID]
Cho EA, Oh HE. Effects of Laughter Therapy on depression, quality of life, resilience and immune responses in breast cancer survivors. J Korean Acad Nurs. 2011; 41(3):285-93. [DOI:10.4040/jkan.2011.41.3.285] [PMID]
Ghodsbin F, Ahmadi ZS, Jahanbin I, Sharif F. The effects of Laughter Therapy on general health of elderly people referring to Jahandidegan community center in Shiraz, Iran, 2014: A randomized controlled trial. Int J Community Based Nurs Midwifery. 2015; 3(1):31-8. [PMID] [PMCID]
Bayat S, Jafari A, Behboodi M. [Effect of Laughter Therapy and physical activity on feelings of loneliness happiness of the elderly (Persian)]. Behav Sci. 2013; 6(20):65-82.
Goldberg DP, Hillier VF. A scaled version of General Health Questionnaire. Psychol Med. 1979; 9(1):131-45. [DOI:10.1017/S0033291700021644]
Malakooti SK, Mirabzadeh A, Fathollahi P, Salavati M, Kahali SH, Afhamebrahimi A, et al. Evolution of reliability, validity and factor analysis of 28 items on the general health of the elderly in Iran (CHQ). Aging. 2006; 1(1):11-21.
De Leo D, Diekstra RF, Lonnqvist J, Lonnqvist J, Cleiren MH, Frisoni GB, et al. LEIPAD, an internationally applicable instrument to assess Quality of life in the elderly. Behav Med. 1998; 24(1):17-27. [DOI:10.1080/08964289809596377] [PMID]
Sajjadi H, Biglareen A. [The Quality of Life of the elderly woman in the Kahrizak (Persian)]. Payesh. 2007; 6(2):105-8.
Ashtiani A, Dastani M. [Psychological tests, personality assessment and mental health (Persian)]. Tehran: Besat Publication; 2009.
Memarian A, Sanatkaran A, Bahari SD, Habibi AM. [The effectiveness of Laughter Yoga exercises on anxiety and sleep quality in the elderly suffering from Parkinson’s disease (Persian)]. Aging Psychol. 2017; 3(2):85-96.
Wagner H, Rehmes U, Kohle D, Puta C. Laughing: A demanding exercise for trunk muscles. Mot Behav. 2014; 46(1):33-7. [DOI:10.1080/00222895.2013.844091] [PMID]
Heo EH, Kim S, Park HJ, Kil SY. The effects of a simulated laughter programme on mood, cortisol levels, and health-related quality of life among haemodialysis patients. Complement Ther Clin Pract. 2016; 25(30):1-7. [DOI:10.1016/j.ctcp.2016.07.001] [PMID]
Ripoll MR, Isabel QC. Laughter and positive therapies: Modern approach and practical use in medicine. Revista de Psiquiatría y Salud Mental. 2010; 3(1):27-34. [DOI:10.1016/S2173-5050(10)70006-6]
Kim SH, Kim YH, Kim HJ, Lee SH, SO Y. The effect of Laughter Therapy on depression, anxiety, and stress in patients with breast cancer undergoing radiotherapy. J Korean Oncol Nurs. 2009; 9(2):155-62. [DOI:10.5388/jkon.2011.11.2.155]
Kim SH, Kim YH, Kim HJ. Laughter and Stress Relief in Cancer Patients: A Pilot Study. Evid Based Complement Alternat Med. 2015; 2015(ID 864739):1-6. [DOI:10.1155/2015/864739]
Westburg NG. Hope, laughter, and humor in residents and staff at an assisted living facility. J Ment Health Couns. 2003; 25(1):16-32. [DOI:10.17744/mehc.25.1.g128feq7x21xxbfe]
Chang C, Tsai G, Hsieh CJ. Psychological, immunological and physiological effects of a Laughing Qigong Program (LQP) on adolescents. Complement Ther Med. 2013; 21(6):660-8. [DOI:10.1016/j.ctim.2013.09.004] [PMID]
Elmali H, Akpinar RB. The effect of watching funny and unfunny videos on post-surgical pain levels. Complement Ther Clin Pract. 2017; 26:36-41. [DOI:10.1016/j.ctcp.2016.11.003] [PMID]
Discussion
This study was conducted with the aim of evaluating the effect of Laughter Therapy on QoL of the elderlies living in Astaneh-ye Ashrafiyeh nursing home. Our study results revealed a significant and positive effect of LT on the QoL of subjects. Also, a significant difference was observed between those in the LT group and the control group in terms of QoL. This finding is consistent with the findings of previous studies [14, 15, 17]. Hence, it can be said that LT which included a series of stimulated laughers, breathing and stretching exercises, watching films and reading comic books, influences the QoL of the elderlies in all aspects of physical functioning, depression/anxiety, life satisfaction, and sexual functioning.
Laughter increases the oxygenation of the body cells, strengthens the immune system, increases blood circulation, and creates positive mental health [25]. Different activities of the body such as deep breathing and intense muscle contractions caused by laughter, improve the contraction of the muscles and movement of the respiratory muscles [26]. Heo et al. on studying the effect of laughter on mood, cortisol levels, and QoL, revealed that LT, breathing, stretching exercises, and meditation had a positive effect on cortisol level and mood [27]. Thus, laughter with creating psychological and physiological changes can improve the QoL of the elderly.
Laughing is also a kind of meditation or relaxation. When people laugh, there is no thought in their minds. All the senses of the person are synchronized for the present moment without any effort and then, he or she feels joy, peace, and comfort [25]. Laughter as a psycho-physiological response to humor or any other similar stimuli such as positive feelings or pleasant thoughts is an activity that encourages the individual and leads to personal well-being. It also creates a positive feeling in the person that improves the way of thinking and QoL [28]. Results of Ko and Youn also indicated the positive effect of this intervention [16]. According to Kim et al. study, LT could also considerably reduce depression, anxiety, and stress [29].
Results of the current study also showed that after one month follow up, the LT program was effective in improving the QoL of the elderly people. In explaining this finding, it can be said that the effects of LT program on improving the QoL of elderly people was sustainable and effective. In this regard, a joyful program, movie, humor, and breathing exercises can sustainability reduce depression and anxiety, and increase the level of life satisfaction and physical well-being. Overall, to explain these findings, it can be said that LT as an intervention that combines relaxation, stretching movements, breathing exercise, joking and laughs, reduces depression, anxiety, and stress and increases hope in the elderly [29-31].
In other words, laughter as a coping mechanism is associated with increased self-efficacy and self-esteem and affects mood and depression. It influences hypothalamic-pituitary-adrenal axis via the central nervous system leading to a decrease in cortisol level and thus, a reduction in stress [32]. Moreover, laughter with stimulation of endorphin production increases the toleration to physical pain, and with increasing the contraction of facial muscles, blood flow, and adrenaline release in the blood increase happiness and joy [33]. The desirable outcome in such situation will be an improvement in QoL.
The results of this study indicate the effectiveness of Laughter Therapy on the quality of life of older people. To achieve more accurate results, it is recommended that future studies be conducted on the older people who do not live in nursing homes. Also, the effectiveness of the LT program can be investigated among the elderly with physical illnesses and their attitudes towards death and themselves. It should be noted that the present study had some limitations. For example, the study population was limited to one nursing home and some subjects were unable to complete the questionnaire due to their senility and low literacy level.
Conclusion
Considering the effectiveness of Laughter Therapy, it is possible to improve the quality of life of the elderly by applying this program. Hence, it is suggested that this program is used in the elderly nursing homes. Furthermore, due to the safety of this program and lack of any adverse effects on the elderly, authorities should consider the Laughter Therapy program as a complementary therapeutic approach along with other therapies to improve the quality of life of the elderly.
Ethical Considerations
Compliance with ethical guidelines
For considering ethical guidelines, the purpose of the study was explained to the participants and they were assured of the confidentiality of their information. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.For considering ethical guidelines, the purpose of the study was explained to the participants and they were assured of the confidentiality of their information.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
Draft: Shima Poorabolghasem Hosseini; Writing–review & editing: Sajjad Rezaei; Resources: All authors; Supervision: Seyed Valiollah Mousavi; and data collecting: Maryana Mahfeli.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
We appreciate the principal of Mehr Aein Nursing Home in Astaneh-ye Ashrafiyeh City (Northern Iran).
References
Khezri Moghadam N, Vahidi S, Ashormahani M. Efficiency of cognitive-existential group therapy on life expectancy and depression of elderly residing in nursing homes. Ageing. 2018; 13(1):62-73. [DOI:10.21859/sija.13.1.62]
Moatamedy A, Borjali A, Sadeqpur M. Prediction of psychological well-being of the elderly based on the power of stress management and social support. Ageing. 2018; 13(1):98-109. [DOI:10.21859/sija.13.1.98]
Mendoza-Nú-ez VM, Sarmiento-Salmorán E, Cortés RC, Maldonado MM, Ruiz-Ramos M. Influence of the self-perception of old age on the effect of a healthy aging program. J Clin Med. 2018; 7(106):1-11.
Saffarinia M, Dortaj A. Effect of group logotherapy on life expectancy and mental and social wellbeing of the female elderly residents of nursing homes in Dubai. Ageing. 2018; 12(4):482-93. [DOI:10.21859/sija.12.4.482]
Kuok K, Li L, Xiang YT, Nogueira BOCL, Ungvari GS, Ng CH, et al. Quality of Life and clinical correlates in older adults living in the community and in nursing homes in Macao. Psychogeriatr. 2017; 17(3):194-9. [DOI:10.1111/psyg.12214]
Canuto A, Weber K, Baertschi M, Andreas S, Volkert J, Dehoust MC, et al. Anxiety disorders in old age: psychiatric comorbidities, quality of life, and prevalence according to age, gender, and country. Am J Geriatr Psychiatry. 2018; 26(2):174-85. [DOI:10.1016/j.jagp.2017.08.015]
Becker NB, Jesus SN, Viseu JN, Stobäus CD, Guerreiro M, Domingues RB. Depression and quality of life in older adults: Mediation effect of sleep quality. Int J Clin Health Psychol. 2018; 18(1):8-17. [DOI:10.1016/j.ijchp.2017.10.002] [PMID] [PMCID]
World Health Organization. WHOQOL: Measuring Quality of Life. Geneva: World Health Organization; 2017.
Gonot-Schoupinsky FN, Garip G. Laughter and humour interventions for well-being in older adults: A systematic review and intervention classification. Complement Ther Med. 2018; 38:85-91. [DOI:10.1016/j.ctim.2018.04.009] [PMID]
Kataria M. Laugh for no reason. Mumbai: Madhuri International; 2005.
Schutzer KA, Graves BS. Barriers and motivations to exercise in older adults. Prev Med. 2004; 39(5):1056-61. [DOI:10.1016/j.ypmed.2004.04.003] [PMID]
Yen HY, Lin LJ. Quality of life in older adults: Benefits from the productive engagement in physical activity. J Exerc Sci Fit. 2018; 16(2):49-54. [DOI:10.1016/j.jesf.2018.06.001] [PMID] [PMCID]
Rezaei S, Montazar E, Mousavi SV, Poorabolghasem Hosseini Sh. Physical Activity and Cognitive Function in the Elderly Population. Caspian J Neurol Sci. 2018; 4(3):121-7.
Kuru N, Kublay G. The effect of Laughter Therapy on the quality of life of nursing home residents. J Clin Nurs. 2017; 26(21-22):3354-62. [DOI:10.1111/jocn.13687] [PMID]
Lebowitz KR, Suh S, Diaz PT, Emery CF. Effects of humor and laughter on psychological functioning, Quality of Life, health status, and pulmonary functioning among patients with chronic obstructive pulmonary disease: A preliminary investigation. Heart Lung. 2011; 40(4):310-9. [DOI:10.1016/j.hrtlng.2010.07.010] [PMID]
Ko HJ, Youn CH. Effects of Laughter Therapy on depression, cognition and sleep among the community‐dwelling elderly. Geriatr Gerontol Int. 2011; 11(3):267-74. [DOI:10.1111/j.1447-0594.2010.00680.x] [PMID]
Cho EA, Oh HE. Effects of Laughter Therapy on depression, quality of life, resilience and immune responses in breast cancer survivors. J Korean Acad Nurs. 2011; 41(3):285-93. [DOI:10.4040/jkan.2011.41.3.285] [PMID]
Ghodsbin F, Ahmadi ZS, Jahanbin I, Sharif F. The effects of Laughter Therapy on general health of elderly people referring to Jahandidegan community center in Shiraz, Iran, 2014: A randomized controlled trial. Int J Community Based Nurs Midwifery. 2015; 3(1):31-8. [PMID] [PMCID]
Bayat S, Jafari A, Behboodi M. [Effect of Laughter Therapy and physical activity on feelings of loneliness happiness of the elderly (Persian)]. Behav Sci. 2013; 6(20):65-82.
Goldberg DP, Hillier VF. A scaled version of General Health Questionnaire. Psychol Med. 1979; 9(1):131-45. [DOI:10.1017/S0033291700021644]
Malakooti SK, Mirabzadeh A, Fathollahi P, Salavati M, Kahali SH, Afhamebrahimi A, et al. Evolution of reliability, validity and factor analysis of 28 items on the general health of the elderly in Iran (CHQ). Aging. 2006; 1(1):11-21.
De Leo D, Diekstra RF, Lonnqvist J, Lonnqvist J, Cleiren MH, Frisoni GB, et al. LEIPAD, an internationally applicable instrument to assess Quality of life in the elderly. Behav Med. 1998; 24(1):17-27. [DOI:10.1080/08964289809596377] [PMID]
Sajjadi H, Biglareen A. [The Quality of Life of the elderly woman in the Kahrizak (Persian)]. Payesh. 2007; 6(2):105-8.
Ashtiani A, Dastani M. [Psychological tests, personality assessment and mental health (Persian)]. Tehran: Besat Publication; 2009.
Memarian A, Sanatkaran A, Bahari SD, Habibi AM. [The effectiveness of Laughter Yoga exercises on anxiety and sleep quality in the elderly suffering from Parkinson’s disease (Persian)]. Aging Psychol. 2017; 3(2):85-96.
Wagner H, Rehmes U, Kohle D, Puta C. Laughing: A demanding exercise for trunk muscles. Mot Behav. 2014; 46(1):33-7. [DOI:10.1080/00222895.2013.844091] [PMID]
Heo EH, Kim S, Park HJ, Kil SY. The effects of a simulated laughter programme on mood, cortisol levels, and health-related quality of life among haemodialysis patients. Complement Ther Clin Pract. 2016; 25(30):1-7. [DOI:10.1016/j.ctcp.2016.07.001] [PMID]
Ripoll MR, Isabel QC. Laughter and positive therapies: Modern approach and practical use in medicine. Revista de Psiquiatría y Salud Mental. 2010; 3(1):27-34. [DOI:10.1016/S2173-5050(10)70006-6]
Kim SH, Kim YH, Kim HJ, Lee SH, SO Y. The effect of Laughter Therapy on depression, anxiety, and stress in patients with breast cancer undergoing radiotherapy. J Korean Oncol Nurs. 2009; 9(2):155-62. [DOI:10.5388/jkon.2011.11.2.155]
Kim SH, Kim YH, Kim HJ. Laughter and Stress Relief in Cancer Patients: A Pilot Study. Evid Based Complement Alternat Med. 2015; 2015(ID 864739):1-6. [DOI:10.1155/2015/864739]
Westburg NG. Hope, laughter, and humor in residents and staff at an assisted living facility. J Ment Health Couns. 2003; 25(1):16-32. [DOI:10.17744/mehc.25.1.g128feq7x21xxbfe]
Chang C, Tsai G, Hsieh CJ. Psychological, immunological and physiological effects of a Laughing Qigong Program (LQP) on adolescents. Complement Ther Med. 2013; 21(6):660-8. [DOI:10.1016/j.ctim.2013.09.004] [PMID]
Elmali H, Akpinar RB. The effect of watching funny and unfunny videos on post-surgical pain levels. Complement Ther Clin Pract. 2017; 26:36-41. [DOI:10.1016/j.ctcp.2016.11.003] [PMID]
Type of Study: Research |
Subject:
Special
Received: 2018/07/5 | Accepted: 2018/11/13 | Published: 2019/01/1
Received: 2018/07/5 | Accepted: 2018/11/13 | Published: 2019/01/1
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
