Fri, Apr 26, 2024
Volume 4, Issue 3 (Summer 2018)
Caspian J Neurol Sci 2018, 4(3): 121-127 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rezaei S, Montazar E, Mousavi S V, Poorabolghasem Hosseini S. Physical Activity and Cognitive Function in the Elderly Population. Caspian J Neurol Sci 2018; 4 (3) :121-127
URL: http://cjns.gums.ac.ir/article-1-237-en.html
URL: http://cjns.gums.ac.ir/article-1-237-en.html



1- Department of Psychology, Faculty of Literature and Humanities, University of Guilan, Rasht, Iran , rezaei_psy@hotmail.com
2- Department of Psychology, Faculty of Literature and Humanities, University of Guilan, Rasht, Iran
2- Department of Psychology, Faculty of Literature and Humanities, University of Guilan, Rasht, Iran
Full-Text [PDF 1182 kb]
(1135 Downloads)
| Abstract (HTML) (4195 Views)

Full-Text: (1331 Views)
Introduction
Aging is not a pathological disorder, but it limits and impacts entire physical and mental activity. During this period, many changes in motor tasks are observed due to disorders in musculoskeletal system and body composition as well as psychological factors associated with aging [1]. In this period, a considerable reduction in muscle size and strength occurs called “Sarcopenia” which causes weakness, reduced mobility and functional autonomy, decreased quality of life, decreased stability, and increased risk of falling and mortality in the elderly [2].
Along with deteriorating changes in physiological and psychological functions, impaired functioning of the elderly, especially their nervous system increases. Also, because of the reduced speed of neurotransmitters and decreased brain volume and flexibility of neuronal cells, a major reduction in cognitive functions is observed in the elderly people [3]. Maintaining an active lifestyle plays a major role in improving the physical abilities of the elderly as it causes compatibility in different physical systems, providing oxygen and nutrients into cells, and improving the metabolic process, especially glucose regulation [4, 5].
Physical activity is defined as voluntary body movements which are produced by muscles and increase the energy consumption. These include activities performed as a part of daily life, such as walking, shopping, and climbing stairs. It is a behavioral factor related to the elderly people’ health and has a positive effect in reducing anxiety, stress, depression; maintaining mental health; and promoting quality of life [6]. Increasing age correlates with brain atrophy and loss of brain volume, i.e. it predicts brain deterioration and cognitive problems in old age. According to studies, lower to moderate level physical activity reduces the risk of cognitive impairment by 35% in people over 65 years old. It increases cell proliferation and cell longevity as well as the production of neurotransmitters in different neurological regions involved in cognitive functions [7, 8].
Epidemiological studies indicate that physical activity may play an important role in maintaining cognitive function throughout life and prevent cognitive deficits [9]. The elderly people who are constantly engaged in daily physical activities have significantly reduced age-related functional attenuation [10]. Findings of Loprinzi, Loprinzi et al., Van Uem et al., Brown et al. and Lerche et al. support a relationship between moderate physical activity and improving cognitive functions in the elderly with a disease as well as healthy ones [11-15].
There is limited information on how physical activity affects the prevention of cognitive problems as well as its relationship with cognitive function, especially in old age. However, we need to know how much and how long the physical activity is required to prevent cognitive impairments in aging. In this regard, this study was conducted to examine the relationship between Physical Activity (PA) and Cognitive Function (CF) in the elderly. Also we attempted to explain cognitive functions with respect to different levels of physical activity.
Materials and Methods
This is a cross-sectional study with descriptive correlational design. Study population consists of all elderly people aged 65 years or above living in Mashhad City, Iran who were members of retirement clubs during 2016-2017. Of these, 200 people aged 65-89 years were selected as study samples using purposeful sampling method. The sample size (97 males, 103 females) was determined in G*Power application according to the F value in ANCOVA analysis, the main effects of different levels of physical activity (low, moderate, and high), considering a maximum of three covariates, 95% confidence interval, 80% test power, and an average effect size of 0.25 [16].
The inclusion criteria were as follows: having an age of 65-90 years, having informed consent, lacking cognitive impairment (such as Alzheimer and vascular dementia) or acute physical-psychological illnesses based on medical records. The exclusion criteria were lacking cooperation; having speech, hearing, or vision problems; and bringing no hearing aids or glasses. For collecting data from the participants, International Physical Activity Questionnaires (IPAQ), and Montreal Cognitive Assessment (MoCA) tools were employed along with a demographic questionnaire. The participants first answered the demographic questions including age, gender, educational degree, and then other questions. But before the study, the participants were assured of the confidentiality of their information.
Study measures
IPAQ assesses PA in five domains of job, transportation, recreation, housework or related works in fields like as walking, moderate and hard chores. Results of PA are reported as MET-minutes/week, where 1 MET (metabolic equivalent) is equal to the energy consumption at 1 min rest. All physical activities can be categorized as coefficients of energy consumption at resting mode. In this questionnaire, the mild PA is 3.3 METs, moderate PA is 4.0 METs and high PA is 8.0 METs. To measure the total PA in a week, the amount of walking (MET×min×d) and the amount of moderate PA (MET×min×d), and high PA (MET×min×d) in the previous week are summed up. IPAQ categorizes PA scores as low (<600 MET), moderate (600–3000 MET) and high (>3000 MET) (IPAQ Research Committee). This tool has been already used in many studies and its validity and reliability have been approved [17].
MoCA with 30 items is widely used for detecting cognitive impairments in eight domains: short-term memory (delayed recall), visio-spatial skills (drawing cube, clock drawing), executive functions (digit and letter span, verbal fluency, abstraction), attention, concentration, working memory (deleting, subtraction, counting), language (naming, sentence repetition), and orientation to time and place. MoCA scores range between 0 and 30. A score of 26 or over is considered to be normal CF, and score of less than 26 indicates cognitive impairments [18]. The reliability and concurrent validity of the Persian version of this instrument have been reported as 0.77 and 0.79, respectively [19].
The collected data were analyzed in SPSS V. 20 considering the significant level of P<0.05. The Pearson correlation test was used to determine the relationship between total IPAQ and MoCA scores. After controlling intervening variables (demographic variables), hierarchical regression analysis was used to examine the predictability of CF based on PA. Furthermore, 1-way ANCOVA was employed to determine differences between CF scores in three PA levels.
Aging is not a pathological disorder, but it limits and impacts entire physical and mental activity. During this period, many changes in motor tasks are observed due to disorders in musculoskeletal system and body composition as well as psychological factors associated with aging [1]. In this period, a considerable reduction in muscle size and strength occurs called “Sarcopenia” which causes weakness, reduced mobility and functional autonomy, decreased quality of life, decreased stability, and increased risk of falling and mortality in the elderly [2].
Along with deteriorating changes in physiological and psychological functions, impaired functioning of the elderly, especially their nervous system increases. Also, because of the reduced speed of neurotransmitters and decreased brain volume and flexibility of neuronal cells, a major reduction in cognitive functions is observed in the elderly people [3]. Maintaining an active lifestyle plays a major role in improving the physical abilities of the elderly as it causes compatibility in different physical systems, providing oxygen and nutrients into cells, and improving the metabolic process, especially glucose regulation [4, 5].
Physical activity is defined as voluntary body movements which are produced by muscles and increase the energy consumption. These include activities performed as a part of daily life, such as walking, shopping, and climbing stairs. It is a behavioral factor related to the elderly people’ health and has a positive effect in reducing anxiety, stress, depression; maintaining mental health; and promoting quality of life [6]. Increasing age correlates with brain atrophy and loss of brain volume, i.e. it predicts brain deterioration and cognitive problems in old age. According to studies, lower to moderate level physical activity reduces the risk of cognitive impairment by 35% in people over 65 years old. It increases cell proliferation and cell longevity as well as the production of neurotransmitters in different neurological regions involved in cognitive functions [7, 8].
Epidemiological studies indicate that physical activity may play an important role in maintaining cognitive function throughout life and prevent cognitive deficits [9]. The elderly people who are constantly engaged in daily physical activities have significantly reduced age-related functional attenuation [10]. Findings of Loprinzi, Loprinzi et al., Van Uem et al., Brown et al. and Lerche et al. support a relationship between moderate physical activity and improving cognitive functions in the elderly with a disease as well as healthy ones [11-15].
There is limited information on how physical activity affects the prevention of cognitive problems as well as its relationship with cognitive function, especially in old age. However, we need to know how much and how long the physical activity is required to prevent cognitive impairments in aging. In this regard, this study was conducted to examine the relationship between Physical Activity (PA) and Cognitive Function (CF) in the elderly. Also we attempted to explain cognitive functions with respect to different levels of physical activity.
Materials and Methods
This is a cross-sectional study with descriptive correlational design. Study population consists of all elderly people aged 65 years or above living in Mashhad City, Iran who were members of retirement clubs during 2016-2017. Of these, 200 people aged 65-89 years were selected as study samples using purposeful sampling method. The sample size (97 males, 103 females) was determined in G*Power application according to the F value in ANCOVA analysis, the main effects of different levels of physical activity (low, moderate, and high), considering a maximum of three covariates, 95% confidence interval, 80% test power, and an average effect size of 0.25 [16].
The inclusion criteria were as follows: having an age of 65-90 years, having informed consent, lacking cognitive impairment (such as Alzheimer and vascular dementia) or acute physical-psychological illnesses based on medical records. The exclusion criteria were lacking cooperation; having speech, hearing, or vision problems; and bringing no hearing aids or glasses. For collecting data from the participants, International Physical Activity Questionnaires (IPAQ), and Montreal Cognitive Assessment (MoCA) tools were employed along with a demographic questionnaire. The participants first answered the demographic questions including age, gender, educational degree, and then other questions. But before the study, the participants were assured of the confidentiality of their information.
Study measures
IPAQ assesses PA in five domains of job, transportation, recreation, housework or related works in fields like as walking, moderate and hard chores. Results of PA are reported as MET-minutes/week, where 1 MET (metabolic equivalent) is equal to the energy consumption at 1 min rest. All physical activities can be categorized as coefficients of energy consumption at resting mode. In this questionnaire, the mild PA is 3.3 METs, moderate PA is 4.0 METs and high PA is 8.0 METs. To measure the total PA in a week, the amount of walking (MET×min×d) and the amount of moderate PA (MET×min×d), and high PA (MET×min×d) in the previous week are summed up. IPAQ categorizes PA scores as low (<600 MET), moderate (600–3000 MET) and high (>3000 MET) (IPAQ Research Committee). This tool has been already used in many studies and its validity and reliability have been approved [17].
MoCA with 30 items is widely used for detecting cognitive impairments in eight domains: short-term memory (delayed recall), visio-spatial skills (drawing cube, clock drawing), executive functions (digit and letter span, verbal fluency, abstraction), attention, concentration, working memory (deleting, subtraction, counting), language (naming, sentence repetition), and orientation to time and place. MoCA scores range between 0 and 30. A score of 26 or over is considered to be normal CF, and score of less than 26 indicates cognitive impairments [18]. The reliability and concurrent validity of the Persian version of this instrument have been reported as 0.77 and 0.79, respectively [19].
The collected data were analyzed in SPSS V. 20 considering the significant level of P<0.05. The Pearson correlation test was used to determine the relationship between total IPAQ and MoCA scores. After controlling intervening variables (demographic variables), hierarchical regression analysis was used to examine the predictability of CF based on PA. Furthermore, 1-way ANCOVA was employed to determine differences between CF scores in three PA levels.
Results
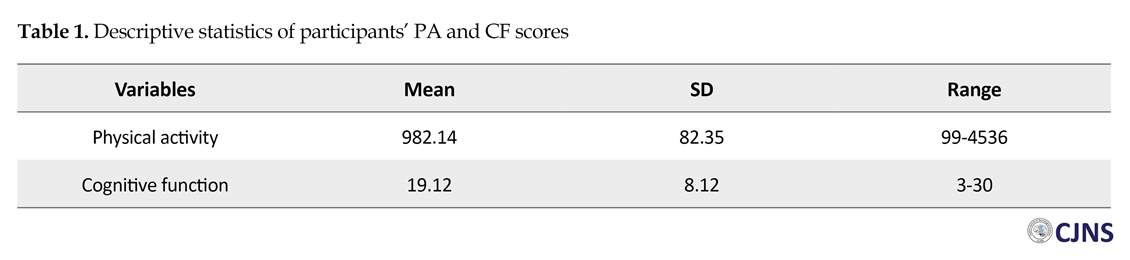
Of 200 participants, 97 (48.5%) were males and 103 (51.5%) were females with a mean age of 65.99 years. Their mean years of study was 6.19 years ranged between 2 and 14 years. Table 1 presents mean and standard deviation of IPAQ and MoCA scores. The Pearson correlation test results indicate that PA has a significant relationship with CF (r=0.63, P<0.0001). This means that with the increase in IPAQ score, the MoCA score increases in the elderly people.
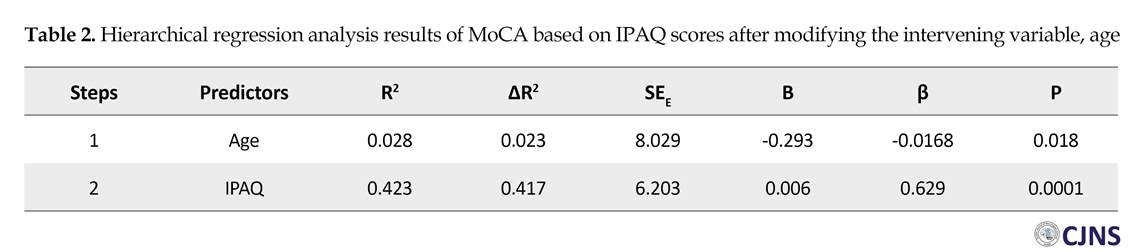
In order to identify intervening variables, the correlation between demographic factors and dependent variable (CF) was evaluated. The results of Pearson correlation coefficients indicated a significant and negative association between age and MoCA score (r=-0.16, P=0.018). i.e. with the increase of age, MoCA scores decreases. No relation was found between educational level and CF (r=-0.073, P=0.306). Results of Independent student t test also showed no significant difference between older men and women in term of MoCA scores (t=0.471, df=198, P=0.638). Therefore, age variable was considered as an intervening variable in this study and its effect on MoCA scores was statistically assessed in hierarchical regression analysis and one-way ANCOVA. Table 2 presents the results of hierarchical regression analysis.
The results of Durbin-Watson test (DW=1.814) indicate that the assumption of the independence of errors was met for performing regression analysis. According to the results in Table 2, after identifying age factor as the control variable, R2 and adjusted R2 coefficients of the model were dramatically improved so that in the second step, about 42% of the changes in MoCA scores can be explained by IPAQ scores (F2,197=72.17, P<0.0001). With regard to the beta coefficient of the predictive variable, with one unit increase in standard deviation of IPAQ score, the standard deviation of MoCA score increases 0.63 unit. With regard to the results and cutoff points of IPAQ, it was found out that the number of people with low energy consumption was 100 (50%), moderate consumption, 89 (44.5%) people and vigorous was 11 (5.5%) people.
Of 200 participants, 97 (48.5%) were males and 103 (51.5%) were females with a mean age of 65.99 years. Their mean years of study was 6.19 years ranged between 2 and 14 years. Table 1 presents mean and standard deviation of IPAQ and MoCA scores. The Pearson correlation test results indicate that PA has a significant relationship with CF (r=0.63, P<0.0001). This means that with the increase in IPAQ score, the MoCA score increases in the elderly people.
In order to identify intervening variables, the correlation between demographic factors and dependent variable (CF) was evaluated. The results of Pearson correlation coefficients indicated a significant and negative association between age and MoCA score (r=-0.16, P=0.018). i.e. with the increase of age, MoCA scores decreases. No relation was found between educational level and CF (r=-0.073, P=0.306). Results of Independent student t test also showed no significant difference between older men and women in term of MoCA scores (t=0.471, df=198, P=0.638). Therefore, age variable was considered as an intervening variable in this study and its effect on MoCA scores was statistically assessed in hierarchical regression analysis and one-way ANCOVA. Table 2 presents the results of hierarchical regression analysis.
The results of Durbin-Watson test (DW=1.814) indicate that the assumption of the independence of errors was met for performing regression analysis. According to the results in Table 2, after identifying age factor as the control variable, R2 and adjusted R2 coefficients of the model were dramatically improved so that in the second step, about 42% of the changes in MoCA scores can be explained by IPAQ scores (F2,197=72.17, P<0.0001). With regard to the beta coefficient of the predictive variable, with one unit increase in standard deviation of IPAQ score, the standard deviation of MoCA score increases 0.63 unit. With regard to the results and cutoff points of IPAQ, it was found out that the number of people with low energy consumption was 100 (50%), moderate consumption, 89 (44.5%) people and vigorous was 11 (5.5%) people.
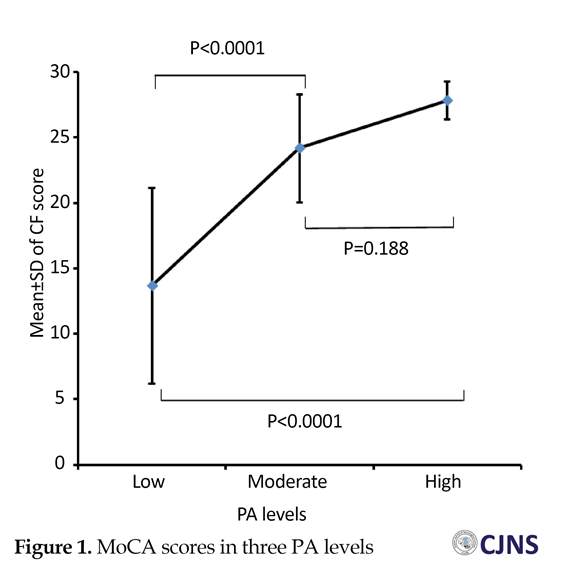
Table 3 presents ANCOVA results of MoCA scores considering three PA levels after controlling the age intervening variable. Before conducing ANCOVA, Levene’s test results showed that the assumption of the equality of variances had been observed (P>0.05). ANCOVA results showed a significant difference between the three groups of elderly with different PA levels (low, moderate, and high) in terms of CF score (F2,196=82.39, P<0.0001).
In order to reveal which groups had a significant difference, the Games-Howell post-hoc test was used for paired comparisons, because it performs better than other post-hoc tests when the sample size between the groups is uneven and very different [20]. Figure 1 plots the differences of MoCA scores in three groups with low, moderate, and high PA. lPMoCAsignificantly lP; the difference is in favor of high PA. However, there was no significant difference between moderate and high PA (P=0.188).
Discussion
The results of the research showed a positive and significant correlation between PA and CF. That is, with the increase in PA, the elderly’s CF increases, too. This indicates that the PA of the elderly at home and at work, in doing sports and leisure-time activities associates with the improvement of their CF in terms of short-term memory, visio-spatial skills, executive functions, attention, concentration, working memory, language, and orientation to time and place. Loprinzi, Loprinziet al., Van Uem et al., Brown et al. also reported a relationship between PA and CF in the elderly [11-14]. Erickson et al. showed that moderate PA is associated with increased CF, especially executive functions [8]. Their longitudinal study indicated that self-reported PA was associated with a 40% reduction in the risk of cognitive problems.
The results of our study also showed difference between the CF of the elderly and different levels of PA (low, moderate, and high). Those with low PA had more cognitive impairment than those with moderate and high PA; however, there was no significant difference between the two groups with moderate and high PA in term of CF score. It indicates that if the elderly has a moderate PA, they can be protected against cognitive impairments. Therefore, balanced PA is necessary to increase the natural capacity of the brain and its flexibility and improve CF and reduce the risk of dementia. Results of Kimura et al. [10] revealed that the elderly people with high PA significantly showed less functional attenuation of prefrontal activations during task-switching reaction time.
Regarding the relationship between PA and CF in the elderly and their better CF with moderate and high PA, it can be said that PA increases energy consumption during consciousness and improves CFs such as executive function and working memory [21]. Longitudinal studies have shown that high PA is correlated with increasing volume in the regions of hippocampus, frontal cortex, and caudate nucleus, which is associated with decreasing risk of cognitive impairments [8]. Also, the findings have shown that regular PA, from 6 months to one year, is associated with greater hippocampal and prefrontal cortex size, indicating the long-term protective effects of PA on CF [22].
Tian et al. showed that PA has correlation with white matter volume in frontoparietal and subcortical networks [23]. Regarding the role of PA in brain function, studies have shown that PA is more associated with increasing neurological efficacy in hippocampus, prefrontal, and cingulate regions during cognitive challenging activities [8]. Therefore, according to the results of the current study and the previous studies, PA affects the structure and function of the brain.
The elderly (naturally and inevitably), with the increase of age, are faced with atrophy and reduced brain volume resulting in functional problems; however, with restorative methods such as PA, they can slow down this declining process. Regular and long-term physical activity with increased volume of frontal and prefrontal area as well as subcortical networks such as hippocampus, caudate nucleus and cingulate regions help improve brain function, enhance performance in cognitive tasks like visio-spatial skills, executive function, attention, concentration, working memory, and language.
This study was limited to a specific region of Iran (northeast part) and the statistical population of the study only consisted of the members of retirement clubs. This fact reduces the generalizability of the results. Also, because of the cross-sectional nature of the research, the data cannot infer causality. Therefore, it is suggested to use larger samples and conduct longitudinal studies for better generalizability.
Given that the results indicated a direct and positive relationship between PA and CF of the elderly, for improving CF (which plays an important role in life and independent performance of the elderly), it is recommended that measures be taken for building facilities such as designing health roads and walking paths. Moreover, it is imperative to increase the public awareness of the elderly and their families about the benefits of PA and its effects on physical and mental health, which encourages more PA in the workplace, home, entertainment and sports.
Conclusion
It was found out that the elderly with a moderate to high PA showed better CF. These results highlight the importance of interventions to increase PA because of its role in physical health, brain structure and function, and thus the improvement of CF in the elderly.
Ethical Considerations
Compliance with ethical guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.
Funding
The authors confirm that they do not have any financial dependency to any organizations, and they have discussed the article topic eagerly.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgements
We appreciate all the people who helped us in conducting this research, especially the responsible of the retirement associations in Mashhad.
References
In order to reveal which groups had a significant difference, the Games-Howell post-hoc test was used for paired comparisons, because it performs better than other post-hoc tests when the sample size between the groups is uneven and very different [20]. Figure 1 plots the differences of MoCA scores in three groups with low, moderate, and high PA. lPMoCAsignificantly lP; the difference is in favor of high PA. However, there was no significant difference between moderate and high PA (P=0.188).
Discussion
The results of the research showed a positive and significant correlation between PA and CF. That is, with the increase in PA, the elderly’s CF increases, too. This indicates that the PA of the elderly at home and at work, in doing sports and leisure-time activities associates with the improvement of their CF in terms of short-term memory, visio-spatial skills, executive functions, attention, concentration, working memory, language, and orientation to time and place. Loprinzi, Loprinziet al., Van Uem et al., Brown et al. also reported a relationship between PA and CF in the elderly [11-14]. Erickson et al. showed that moderate PA is associated with increased CF, especially executive functions [8]. Their longitudinal study indicated that self-reported PA was associated with a 40% reduction in the risk of cognitive problems.
The results of our study also showed difference between the CF of the elderly and different levels of PA (low, moderate, and high). Those with low PA had more cognitive impairment than those with moderate and high PA; however, there was no significant difference between the two groups with moderate and high PA in term of CF score. It indicates that if the elderly has a moderate PA, they can be protected against cognitive impairments. Therefore, balanced PA is necessary to increase the natural capacity of the brain and its flexibility and improve CF and reduce the risk of dementia. Results of Kimura et al. [10] revealed that the elderly people with high PA significantly showed less functional attenuation of prefrontal activations during task-switching reaction time.
Regarding the relationship between PA and CF in the elderly and their better CF with moderate and high PA, it can be said that PA increases energy consumption during consciousness and improves CFs such as executive function and working memory [21]. Longitudinal studies have shown that high PA is correlated with increasing volume in the regions of hippocampus, frontal cortex, and caudate nucleus, which is associated with decreasing risk of cognitive impairments [8]. Also, the findings have shown that regular PA, from 6 months to one year, is associated with greater hippocampal and prefrontal cortex size, indicating the long-term protective effects of PA on CF [22].
Tian et al. showed that PA has correlation with white matter volume in frontoparietal and subcortical networks [23]. Regarding the role of PA in brain function, studies have shown that PA is more associated with increasing neurological efficacy in hippocampus, prefrontal, and cingulate regions during cognitive challenging activities [8]. Therefore, according to the results of the current study and the previous studies, PA affects the structure and function of the brain.
The elderly (naturally and inevitably), with the increase of age, are faced with atrophy and reduced brain volume resulting in functional problems; however, with restorative methods such as PA, they can slow down this declining process. Regular and long-term physical activity with increased volume of frontal and prefrontal area as well as subcortical networks such as hippocampus, caudate nucleus and cingulate regions help improve brain function, enhance performance in cognitive tasks like visio-spatial skills, executive function, attention, concentration, working memory, and language.
This study was limited to a specific region of Iran (northeast part) and the statistical population of the study only consisted of the members of retirement clubs. This fact reduces the generalizability of the results. Also, because of the cross-sectional nature of the research, the data cannot infer causality. Therefore, it is suggested to use larger samples and conduct longitudinal studies for better generalizability.
Given that the results indicated a direct and positive relationship between PA and CF of the elderly, for improving CF (which plays an important role in life and independent performance of the elderly), it is recommended that measures be taken for building facilities such as designing health roads and walking paths. Moreover, it is imperative to increase the public awareness of the elderly and their families about the benefits of PA and its effects on physical and mental health, which encourages more PA in the workplace, home, entertainment and sports.
Conclusion
It was found out that the elderly with a moderate to high PA showed better CF. These results highlight the importance of interventions to increase PA because of its role in physical health, brain structure and function, and thus the improvement of CF in the elderly.
Ethical Considerations
Compliance with ethical guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.
Funding
The authors confirm that they do not have any financial dependency to any organizations, and they have discussed the article topic eagerly.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgements
We appreciate all the people who helped us in conducting this research, especially the responsible of the retirement associations in Mashhad.
References
- Khezri A, Arab Ameri E, Hemayattalab R, Ebrahimi R. [The Effect of sports and physical activity on elderly reaction time and response time (Persian)]. Iran J Ageing. 2014; 9(2):106-13.
- Valipour Dehnou V, Reza Motamedi R. [assessing and comparing of balance and flexibility among elderly men and women in the age group of 60-79 years (Persian)]. Iran J Ageing. 2018; 13(2):210-21.
- Saint Martin M, Sforza E, Roche F, Barthélémy JC, Thomas-Anterion C. Sleep breathing disorders and cognitive function in the elderly: An 8-year follow-up study. The proof-synapse cohort. sleep. 2015; 38(2):179-87. [DOI:10.5665/sleep.4392]
- McPhee JS, French DP, Jackson D, Nazroo J, Pendleton N, Degens H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontol. 2016; 17(3):567-80. [DOI:10.1007/s10522-016-9641-0] [PMID] [PMCID]
- Juniora RC, Fernandesc TG, Borges GF, Guerra RO, de Abreub DC. Factors associated with low levels of physical activity among elderly residents in a small urban area in the interior of the Brazilian Amazon. Arch Gerontol Geriatr. 2018; 75:37-43. [DOI:10.1016/j.archger.2017.11.007] [PMID]
- Lok N, Lok S, Canbaz M. The effect of physical activity on depressive symptoms and quality of life among elderly nursing home residents: Randomized controlled trial. Arch Gerontol Geriatr. 2017; 70:92-8. [DOI:10.1016/j.archger.2017.01.008]
- Shamsipour Dehkordi P, Mot abadi M. [Interactive role of physical activity and body mass indices levels on cognitive function and psychological well-being of the elderly (Persian)]. J Shahrekord Univ Med Sci. 2017; 19(2):60-75.
- Erickson KI, Hillman CH, Kramer AF. Physical activity, brain, and cognition. Curr Opin Behav Sci. 2015; 4:27-32. [DOI:10.1016/j.cobeha.2015.01.005]
- Tierney MC, Moineddin R, Morra A, Manson J, Blake J. Intensity of recreational physical activity throughout life and later life cognitive functioning in women. J Alzheimers Dis. 2011; 22(4):1331-8. [DOI:10.3233/JAD-2010-101188] [PMID]
- Kimura K, Yasunaga A, Wang L. Correlation between moderate daily physical activity and neurocognitive variability in healthy elderly people. Arch Gerontol Geriatr. 2013; 56(1):109-17. [DOI:10.1016/j.archger.2012.10.004] [PMID]
- Loprinzi PD. Epidemiological investigation of muscle-strengthening activities and cognitive function among older adults. Chronic Illn. 2016; 12(2):157-62. [DOI:10.1177/1742395316641998] [PMID]
- Loprinzi PD, Danzl MM, Ulanowski E, Paydo C. A pilot study evaluating the association between physical activity and cognition among individuals with Parkinson’s disease. Disabil Health J. 2018; 11(1):165-8. [DOI:10.1016/j.dhjo.2017.05.004]
- Van Uem JMT, Cerff B, Kampmeyer M, Prinzen J, Zuidema M, Hobert MA, et al. The association between objectively measured physical activity, depression, cognition, and health-related-quality of life in parkinson’s disease. Parkinsonism Relat Disord. 2018; 48:74-81. [DOI:10.1016/j.parkreldis.2017.12.023]
- Brown BM, Rainey-Smith SR, Castalanelli N, Gordon N, MarkovicSh, Sohrabi H, et al. Study protocol of the Intense Physical Activity and Cognition study: The effect of high-intensity exercise training on cognitive function in older adults. Alzheimers Dement: Transl Res Clin Interv. 2017; 3(4):562-70. [DOI:10.1016/j.trci.2017.09.003] [PMID] [PMCID]
- Lerche S, Gutfreund A, Brockmann K, Hobert MA, Wurster I, S¨unkel U, et al. Effect of physical activity on cognitive flexibility, depression and RBD in healthy elderly. Clin Neurol Neurosurg. 2018; 165:88-93. [DOI:10.1016/j.clineuro.2018.01.008.]
- Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007; 39(2):175-91. [DOI:10.3758/BF03193146] [PMID]
- Craig CL, Marshall AL, Sjorstrom M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Behav Res Methods. 2003; 35(8):1381-95. [DOI:10.1249/01.MSS.0000078924.61453.FB] [PMID]
- Lopez MN, Charter RA, Mostafavi B, Nibut LP. Psychometric properties of the Folstein Mini-Mental State Examination. Assessment. 2005; 12(2):137-44. [DOI:10.1177/1073191105275412] [PMID]
- Emsaki G, Molavi H, Chitsaz A, Abtahi MM, Asgari K. [Psychometric properties of the Montreal Cognitive Assessment (MoCA) in Parkinson’s disease patients in Isfahan (Persian)]. J Isfahan Med Sch. 2011; 29(158):1391-1400.
- Habibpoor K, Safari R. [Comprehensive manual for using SPSS in survey researches (Persian)]. Tehran: Looyeh and Motefakkeran Publication; 2010.
- Wilckens KA, Ferrarelli F, Walker MP, Buysse DJ. Slow-wave activity enhancement to improve cognition. Trends Neurosci. 2018; 41(7):470-82. [DOI:10.1016/j.tins.2018.03.003.]
- Hamilton GF, Rhodes JS. Animal models of exercise–brain interactions. Exerc Cogn Interact. 2016; 43-63. [DOI:10.1016/B978-0-12-800778-5.00003-7]
- Tian Q, Erickson KI, Simonsick EM, Aizenstein HJ, Glynn NW, Boudreau RM, et al. Physical activity predicts microstructural integrity in memoryrelated networks in very old adults. J Gerontol A Biol Sci Med Sci. 2014; 69(10):1284-90. [DOI:10.1093/gerona/glt287] [PMID] [PMCID]
Type of Study: Research |
Subject:
Special
Received: 2018/01/20 | Accepted: 2018/05/25 | Published: 2018/07/1
Received: 2018/01/20 | Accepted: 2018/05/25 | Published: 2018/07/1
References
1. Khezri A, Arab Ameri E, Hemayattalab R, Ebrahimi R. [The Effect of sports and physical activity on elderly reaction time and response time (Persian)]. Iran J Ageing. 2014; 9(2):106-13.
2. Valipour Dehnou V, Reza Motamedi R. [assessing and comparing of balance and flexibility among elderly men and women in the age group of 60-79 years (Persian)]. Iran J Ageing. 2018; 13(2):210-21.
3. Saint Martin M, Sforza E, Roche F, Barthélémy JC, Thomas-Anterion C. Sleep breathing disorders and cognitive function in the elderly: An 8-year follow-up study. The proof-synapse cohort. sleep. 2015; 38(2):179-87. [DOI:10.5665/sleep.4392] [DOI:10.5665/sleep.4392]
4. McPhee JS, French DP, Jackson D, Nazroo J, Pendleton N, Degens H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontol. 2016; 17(3):567-80. [DOI:10.1007/s10522-016-9641-0] [PMID] [PMCID] [DOI:10.1007/s10522-016-9641-0]
5. Juniora RC, Fernandesc TG, Borges GF, Guerra RO, de Abreub DC. Factors associated with low levels of physical activity among elderly residents in a small urban area in the interior of the Brazilian Amazon. Arch Gerontol Geriatr. 2018; 75:37-43. [DOI:10.1016/j.archger.2017.11.007] [PMID] [DOI:10.1016/j.archger.2017.11.007]
6. Lok N, Lok S, Canbaz M. The effect of physical activity on depressive symptoms and quality of life among elderly nursing home residents: Randomized controlled trial. Arch Gerontol Geriatr. 2017; 70:92-8. [DOI:10.1016/j.archger.2017.01.008] [DOI:10.1016/j.archger.2017.01.008]
7. Shamsipour Dehkordi P, Mot abadi M. [Interactive role of physical activity and body mass indices levels on cognitive function and psychological well-being of the elderly (Persian)]. J Shahrekord Univ Med Sci. 2017; 19(2):60-75.
8. Erickson KI, Hillman CH, Kramer AF. Physical activity, brain, and cognition. Curr Opin Behav Sci. 2015; 4:27-32. [DOI:10.1016/j.cobeha.2015.01.005] [DOI:10.1016/j.cobeha.2015.01.005]
9. Tierney MC, Moineddin R, Morra A, Manson J, Blake J. Intensity of recreational physical activity throughout life and later life cognitive functioning in women. J Alzheimers Dis. 2011; 22(4):1331-8. [DOI:10.3233/JAD-2010-101188] [PMID] [DOI:10.3233/JAD-2010-101188]
10. Kimura K, Yasunaga A, Wang L. Correlation between moderate daily physical activity and neurocognitive variability in healthy elderly people. Arch Gerontol Geriatr. 2013; 56(1):109-17. [DOI:10.1016/j.archger.2012.10.004] [PMID] [DOI:10.1016/j.archger.2012.10.004]
11. Loprinzi PD. Epidemiological investigation of muscle-strengthening activities and cognitive function among older adults. Chronic Illn. 2016; 12(2):157-62. [DOI:10.1177/1742395316641998] [PMID] [DOI:10.1177/1742395316641998]
12. Loprinzi PD, Danzl MM, Ulanowski E, Paydo C. A pilot study evaluating the association between physical activity and cognition among individuals with Parkinson's disease. Disabil Health J. 2018; 11(1):165-8. [DOI:10.1016/j.dhjo.2017.05.004] [DOI:10.1016/j.dhjo.2017.05.004]
13. Van Uem JMT, Cerff B, Kampmeyer M, Prinzen J, Zuidema M, Hobert MA, et al. The association between objectively measured physical activity, depression, cognition, and health-related-quality of life in parkinson's disease. Parkinsonism Relat Disord. 2018; 48:74-81. [DOI:10.1016/j.parkreldis.2017.12.023] [DOI:10.1016/j.parkreldis.2017.12.023]
14. Brown BM, Rainey-Smith SR, Castalanelli N, Gordon N, MarkovicSh, Sohrabi H, et al. Study protocol of the Intense Physical Activity and Cognition study: The effect of high-intensity exercise training on cognitive function in older adults. Alzheimers Dement: Transl Res Clin Interv. 2017; 3(4):562-70. [DOI:10.1016/j.trci.2017.09.003] [PMID] [PMCID] [DOI:10.1016/j.trci.2017.09.003]
15. Lerche S, Gutfreund A, Brockmann K, Hobert MA, Wurster I, S¨unkel U, et al. Effect of physical activity on cognitive flexibility, depression and RBD in healthy elderly. Clin Neurol Neurosurg. 2018; 165:88-93. [DOI:10.1016/j.clineuro.2018.01.008.] [DOI:10.1016/j.clineuro.2018.01.008]
16. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007; 39(2):175-91. [DOI:10.3758/BF03193146] [PMID] [DOI:10.3758/BF03193146]
17. Craig CL, Marshall AL, Sjorstrom M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Behav Res Methods. 2003; 35(8):1381-95. [DOI:10.1249/01.MSS.0000078924.61453.FB] [PMID] [DOI:10.1249/01.MSS.0000078924.61453.FB]
18. Lopez MN, Charter RA, Mostafavi B, Nibut LP. Psychometric properties of the Folstein Mini-Mental State Examination. Assessment. 2005; 12(2):137-44. [DOI:10.1177/1073191105275412] [PMID] [DOI:10.1177/1073191105275412]
19. Emsaki G, Molavi H, Chitsaz A, Abtahi MM, Asgari K. [Psychometric properties of the Montreal Cognitive Assessment (MoCA) in Parkinson's disease patients in Isfahan (Persian)]. J Isfahan Med Sch. 2011; 29(158):1391-1400.
20. Habibpoor K, Safari R. [Comprehensive manual for using SPSS in survey researches (Persian)]. Tehran: Looyeh and Motefakkeran Publication; 2010.
21. Wilckens KA, Ferrarelli F, Walker MP, Buysse DJ. Slow-wave activity enhancement to improve cognition. Trends Neurosci. 2018; 41(7):470-82. [DOI:10.1016/j.tins.2018.03.003.] [DOI:10.1016/j.tins.2018.03.003]
22. Hamilton GF, Rhodes JS. Animal models of exercise–brain interactions. Exerc Cogn Interact. 2016; 43-63. [DOI:10.1016/B978-0-12-800778-5.00003-7] [DOI:10.1016/B978-0-12-800778-5.00003-7]
23. Tian Q, Erickson KI, Simonsick EM, Aizenstein HJ, Glynn NW, Boudreau RM, et al. Physical activity predicts microstructural integrity in memoryrelated networks in very old adults. J Gerontol A Biol Sci Med Sci. 2014; 69(10):1284-90. [DOI:10.1093/gerona/glt287] [PMID] [PMCID] [DOI:10.1093/gerona/glt287]
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
