Fri, Sep 20, 2024
Volume 4, Issue 4 (Autumn 2018)
Caspian J Neurol Sci 2018, 4(4): 137-143 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mehvari Habibabadi J, Naghibi N, Falahatian M, Izadi M. The Relationship Between Perceived Social Support and Self-Esteem in Patients With Epilepsy. Caspian J Neurol Sci 2018; 4 (4) :137-143
URL: http://cjns.gums.ac.ir/article-1-226-en.html
URL: http://cjns.gums.ac.ir/article-1-226-en.html



1- Department of Neurology, School of Medicine, Isfahan University of Medical Sciences, Isfahan, Iran
2- Epilepsy Nurse, School of Nursing, Isfahan University of Medical Sciences, Isfahan, Iran
2- Epilepsy Nurse, School of Nursing, Isfahan University of Medical Sciences, Isfahan, Iran
Full-Text [PDF 1039 kb]
(974 Downloads)
| Abstract (HTML) (2839 Views)
Discussion
The current study aimed at investigating the relationship between perceived social support and self-esteem in patients with epilepsy referring to Kashani Hospital in Isfahan from 2017 to 2018. Descriptive findings revealed that the majority of the subjects were female patients (64.9%) and the age range of 26 to 30 years was predominant (33.1%). Results of the study indicated a significant correlation with 99% confidence interval between social support dimensions (including spouse, family members, friends, physician, and nurse) and self-esteem in the studied patients (P<0.001). Also, results of multiple regression analysis showed that spouse support, family members support, friends support, physician support, and nurse support predicted 12.4%, 41.5%, 4.6%, 4.7%, and 16.8% of self-esteem changes, respectively. These variables, in total, could predict about 80% of changes in self-esteem.

The results of the current study showed that most of the patients had high perceived social support. Family members are one of the most important elements of social support for patients, and the highest score among the dimensions of perceived social support belonged to the family members, which had the greatest impact on patients’ self-esteem. The family is the major source of social support for patients with epilepsy. To the best of authors’ knowledge, such findings might be attributed to Iranian culture, as the family members are the major
source of support for individuals, and as advisors, encourage individuals to adapt to the disease.
In a study on 160 patients treated in three different hemodialysis centers, Kara et al. reported the family as the major source of support for patients and suggested that perceived social support can affect the aspects non-adherence to dialysis diet and fluid restrictions [19]. Also, the results of studies demonstrate that social support in patients with heart failure can improve or maintain their quality of life. Janowski et al. found that patients with higher levels of perceived social support had a significantly higher quality of life, lower levels of depression, and higher acceptance of life with psoriasis. Song et al. also stated that social support is an important factor in self-care behaviors of patients with type II diabetes mellitus [20].
The results of the study showed that patients received the lowest level of social support from friends and this dimension had the lowest impact on patients’ self-esteem. One of the reasons for this finding can be the nature of the disease that affects patients’ communication skills. Other studies also showed that social support can improve the quality of life and reduce stress caused by hospitalization. In addition, perceived social support may reduce mortality in patients. In a study on patients undergoing hemodialysis, Welch et al. found that adherence to fluid restrictions was closely associated with social support in such patients [21]. The limitations of the current study were as follows: small sample size and not considering the impact of other social support aspects on self-esteem.

Conclusion
Social support can increase the self-esteem of patients with epilepsy. Increasing the self-esteem of such patients can help with their improvement (as an adjuvant). According to the results of the current study, patients perceived the least amount of social support from friends. One of the reasons for this finding could be the nature of the disease that affects patients’ communication skills. Also, further studies on the relation between social support and self-esteem in larger sample sizes are recommended.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by the Ethics Committee of Isfahan University of Medical Sciences (No. 397365). All the study procedures were in compliance with the ethical guidelines of the Declaration of Helsinki 1957.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
The authors contributions is as follows: Draft: Jafar Mehvari Habibabadi; Writing–review & editing: All authors; Funding acquisition: Jafar Mehvari Habibabadi; Resources: All authors; and Supervision: Jafar Mehvari Habibabadi and Maryam Izadi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Authors hereby wish to thank the Comprehensive Epilepsy Center of Kashani Hospital, Isfahan, Iran.
References
Full-Text: (1088 Views)
Introduction
Epilepsy is one of the most common neurological disorders and serious public health problems, which is also the second cause of neurological diseases in the world after stroke [1]. Epilepsy is a chronic disease, which includes repeated seizure attacks caused by abnormal electrical signals in the brain and involves neurological, cognitive, physiological, and social dimensions [2]. Epilepsy can occur at any age, race, or social class [3]. The number of patients with epilepsy in the United States is about two million and in the United Kingdom is 300,000 [4]. It is reported that 3-5% of the world’s population present seizure attacks during their lifetime and 0.5-1% of the world’s population are affected by active epilepsy [5].
The incidence of epilepsy in the developed and developing countries is 40-70 and 190 per 100,000 individuals, respectively [6]. In most of the countries, the prevalence of active epilepsy is 4-10 per 1000 individuals [1]. Based on a systematic review findings (2014), the prevalence of epilepsy in Iran was 7.87 per 1000 individuals and the number of affected people in 2011 was about 800,000 [7]. According to research articles finings, 1%-1.5% of Iran current population have epilepsy, which indicates that the proportion of patients with epilepsy is about three times higher than that of Europe [7].
The increasing trend of affected people in Iran calls for further attention, which should be paid to the problems and treatment challenges and adaptation to this disease [7]. Patients with epilepsy also have ocular problems, anxiety, depression, and memory impairments. No definitive treatment has been introduced for such patients so far, and about one-third of them have not yet been cured, and also the causes of exacerbation and relief of their disease are not clearly understood [8].
Perception of social support is defined as a mental sensation of belonging, accepting, being interested, and getting help in the required circumstances [9]. Some authors indicated social support as a degree of fulfilling emotional needs, satisfaction, belonging, and security to others [10]. Social support can be provided as psychosocial, emotional, informational, tangible, and interactive support, but the patient’s understanding of the support provided is of great importance. Understanding the benefits of social support can play an important role in the advanced stages of chronic diseases and may protect the individual against the tensions caused by the disease, reduce the negative psychological consequences of physical defects, and ease tolerating the disease throughout enhancing the compatibility [11].
Social support affects health behaviors, as well as disease and treatment outcomes by changing people’s perceptions of stressful life events, such as epilepsy, and reducing negative psychological responses to these stressor factors. Perceiving the social support can prevent physiological adverse effects of the disease, and remain a beneficial impact on physical-psychological symptoms and functioning, and protect individuals from the adverse effects of life crises [12]. Physical illnesses, such as epilepsy, can distort perception of social support, as the patient gradually shifts away from family members and other people and avoids social contacts [13].
Perceived social support is one of the factors that contribute to self-esteem in patients with epilepsy. Patients with epilepsy usually receive little social support, which causes psychological problems, including depression and anxiety and decreased self-esteem [14]. Self-esteem is known as a stress regulator. Therefore, people with higher self-esteem have a higher sense of self-worthiness in stressful situations, which in turn protects them against stress outcomes [14].
Reviewing the literature revealed a huge number of researches on the relationship between self-esteem and perceived social support in some diseases; however, most studies in this regard are conducted on adults or young individuals, as well as patients with cancer or multiple sclerosis. Also, there are limited study on the relationship between self-esteem and perceived social support in patients with epilepsy. Therefore, considering the impact of perceived social support on increasing self-esteem, and reducing the psychological consequences of seizure attacks and treatment complications, the current study aimed at evaluating the relationship between the components of self-esteem and perceived social support in patients with epilepsy for the first time in Iran.
Materials and Methods
The current cross sectional, correlational study was conducted on 211 patients with epilepsy referring to the Neurology Department and Comprehensive Epilepsy Center of Kashani Hospital in Isfahan, Iran from 2017 to 2018. Patients were selected through convenience sampling method and inclusion and exclusion criteria were used to enroll eligible subjects. Kashani Hospital in Isfahan was selected as the research setting because of ease of access to the study samples (simple or consecutive sampling). Diagnosis of epilepsy was confirmed by a epilepsy fellowship based on standard criteria [15] and psychological evaluations were performed by a psychiatric. The inclusion criteria were: having epilepsy and signing the written informed consent; at least six months of definitively being diagnosed with epilepsy and treatment onset; being able to answer the questions; no physical-psychological illnesses.
The exclusion criteria were: incidence of any acute diseases associated with seizure attacks during the data collection; no willingness to participate in the study; being missed to follow-up. The patients were enrolled if they met the inclusion criteria and had the desire for participation. The researchers referred to the study site and introduced themselves, explained the research objectives, provided explanations about the way to complete the questionnaires for patients and obtained the signed written consent forms from the ones who returned completed questionnaires. After obtaining permission from authorities, patients were placed in an appropriate place to complete the questionnaires.
The instrument used in the study was comprised of self-esteem and social support questionnaires and demographic characteristics checklist was also added to the first part. Demographic characteristics included age, gender, marital status, occupational status, educational level, and duration of the disease. The first questionnaire was the Rosenberg self-esteem scale. The content reliability and validity of the Rosenberg self-esteem scale was confirmed based on the comments of the developers and some preliminary studies [16].
The Rosenberg Self-Esteem Scale contains 10 general items that are scored based on a five-point Likert scale from 0 to 3 as: totally disagree (0), disagree (1), agree (2), and totally agree (3), the maximum score of the self-esteem questionnaire is 30. Scores above 25 indicate high self-esteem, 15-25 moderate self-esteem, and less than 15 indicate low self-esteem [17].
The second questionnaire was the social support questionnaire designed based on the Northouse Social Support Questionnaire (SSQ). The content reliability and validity of the SSQ was confirmed in another study [18]. The Northouse SSQ consists of 40 items in five dimensions as spouse, family members, friends, physician, and nurse. Each dimension has eight items that measure the level of social support perceived by patient’s spouse, family members, friends, physician, and nurse. The items are scored based on a five-point Likert scale from 1 to 5 as: totally disagree (1), disagree (2), no idea (3), agree (4), and totally agree (5).
The score of each dimension is separately calculated and the total score, which is calculated by summing the dimensions scores, ranges 40 to 200. The total score of perceived social support is interpreted as follows: low (40-92), moderate (93-146), and high (147-200), and the score of each dimension is also interpreted as: low (8-18), medium (19-29) and high (30-40). It should be noted that items of spouse dimension of are not omitted for single subjects. In addition, the Northouse SSQ has open-ended items to measure the social network of patients that was not applicable to the current study.
In the study, the collected data were analyzed using descriptive and statistical inference with SPSS V. 23. Descriptive statistics including frequency distribution, as well as mean and standard deviation was used to express data. Multiple regression analysis and Pearson Correlation Coefficient were also employed.
Results
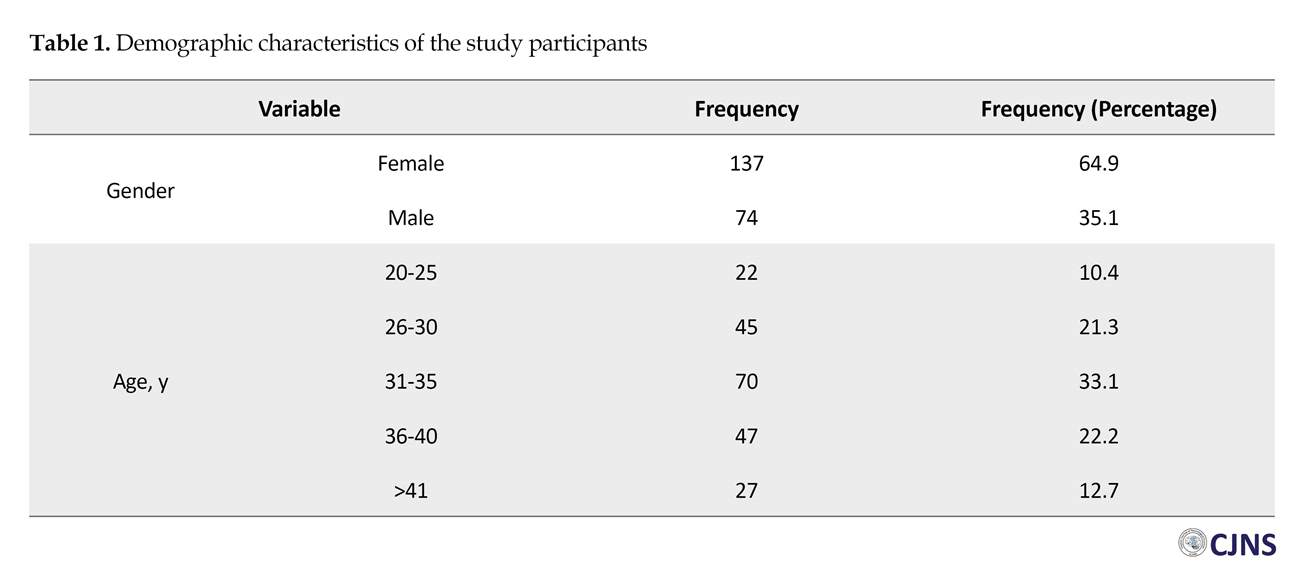
In the present study, 211 patients with epilepsy referring to the Neurology Department and Comprehensive Epilepsy Center of Kashani Hospital were studied and all the participants completed questionnaires (100% response rate). Findings of the demographic variables are summarized in Table 1. The findings showed that 64.92% of the respondents were female and 35.1% male. Regarding the frequency distribution of respondents, in terms of age, the findings indicated that 10.4% of the respondents were within the age range of 20-25 years, 21.3% were 26-30 years, 33.1% were 31-35 years, 22.2% were 36-40 years , and 12.7% were above 41 years (Table 1).
Descriptive indices of the self-esteem score and the perceived social support score in each dimension are shown in Table 2. The findings revealed that the level of perceived social support was high in most of the studied cases and the highest score belonged to the family members’ dimension. The Pearson correlation showed no significant relationship between self-esteem and social support perceived by the spouse, family members, friends, physician, and nurse (P>0.05).
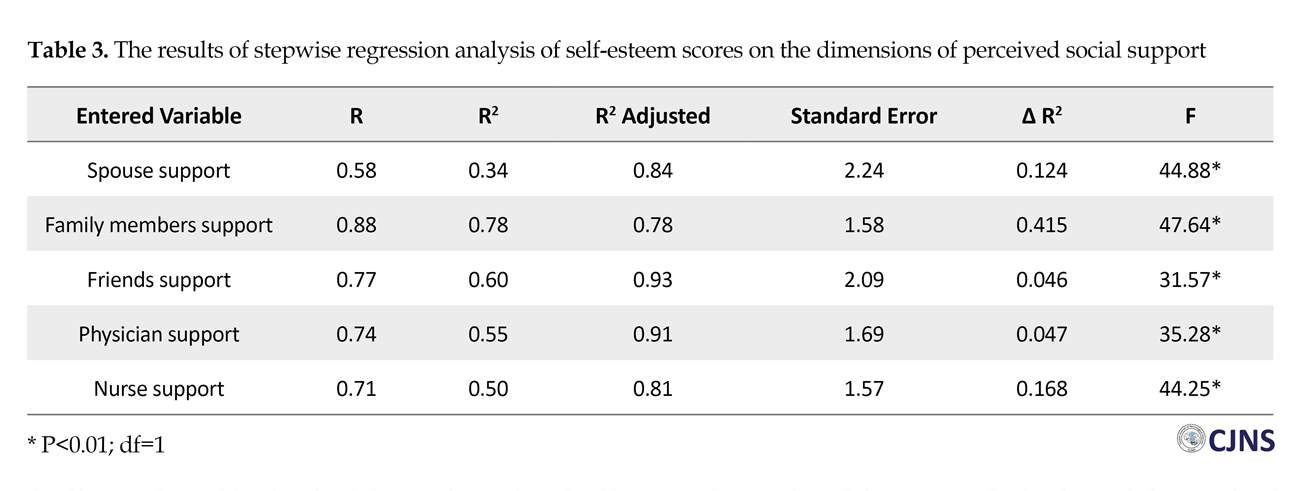
To investigate the prediction of self-esteem variable by perceived social support, the perceived social support components were introduced stepwise to self-esteem variables. Stepwise regression was evaluated and the results are shown on Table 3. All variables significantly retained themselves in five steps. The results of variance analysis showed that social support dimensions including spouse, family members, friends, physician, and nurse had a significant impact on self-esteem. The results of stepwise regression are reported in five steps. As shown in Table 4, the total score of perceived social support and self-esteem had a significant correlation (P<0.001).
Epilepsy is one of the most common neurological disorders and serious public health problems, which is also the second cause of neurological diseases in the world after stroke [1]. Epilepsy is a chronic disease, which includes repeated seizure attacks caused by abnormal electrical signals in the brain and involves neurological, cognitive, physiological, and social dimensions [2]. Epilepsy can occur at any age, race, or social class [3]. The number of patients with epilepsy in the United States is about two million and in the United Kingdom is 300,000 [4]. It is reported that 3-5% of the world’s population present seizure attacks during their lifetime and 0.5-1% of the world’s population are affected by active epilepsy [5].
The incidence of epilepsy in the developed and developing countries is 40-70 and 190 per 100,000 individuals, respectively [6]. In most of the countries, the prevalence of active epilepsy is 4-10 per 1000 individuals [1]. Based on a systematic review findings (2014), the prevalence of epilepsy in Iran was 7.87 per 1000 individuals and the number of affected people in 2011 was about 800,000 [7]. According to research articles finings, 1%-1.5% of Iran current population have epilepsy, which indicates that the proportion of patients with epilepsy is about three times higher than that of Europe [7].
The increasing trend of affected people in Iran calls for further attention, which should be paid to the problems and treatment challenges and adaptation to this disease [7]. Patients with epilepsy also have ocular problems, anxiety, depression, and memory impairments. No definitive treatment has been introduced for such patients so far, and about one-third of them have not yet been cured, and also the causes of exacerbation and relief of their disease are not clearly understood [8].
Perception of social support is defined as a mental sensation of belonging, accepting, being interested, and getting help in the required circumstances [9]. Some authors indicated social support as a degree of fulfilling emotional needs, satisfaction, belonging, and security to others [10]. Social support can be provided as psychosocial, emotional, informational, tangible, and interactive support, but the patient’s understanding of the support provided is of great importance. Understanding the benefits of social support can play an important role in the advanced stages of chronic diseases and may protect the individual against the tensions caused by the disease, reduce the negative psychological consequences of physical defects, and ease tolerating the disease throughout enhancing the compatibility [11].
Social support affects health behaviors, as well as disease and treatment outcomes by changing people’s perceptions of stressful life events, such as epilepsy, and reducing negative psychological responses to these stressor factors. Perceiving the social support can prevent physiological adverse effects of the disease, and remain a beneficial impact on physical-psychological symptoms and functioning, and protect individuals from the adverse effects of life crises [12]. Physical illnesses, such as epilepsy, can distort perception of social support, as the patient gradually shifts away from family members and other people and avoids social contacts [13].
Perceived social support is one of the factors that contribute to self-esteem in patients with epilepsy. Patients with epilepsy usually receive little social support, which causes psychological problems, including depression and anxiety and decreased self-esteem [14]. Self-esteem is known as a stress regulator. Therefore, people with higher self-esteem have a higher sense of self-worthiness in stressful situations, which in turn protects them against stress outcomes [14].
Reviewing the literature revealed a huge number of researches on the relationship between self-esteem and perceived social support in some diseases; however, most studies in this regard are conducted on adults or young individuals, as well as patients with cancer or multiple sclerosis. Also, there are limited study on the relationship between self-esteem and perceived social support in patients with epilepsy. Therefore, considering the impact of perceived social support on increasing self-esteem, and reducing the psychological consequences of seizure attacks and treatment complications, the current study aimed at evaluating the relationship between the components of self-esteem and perceived social support in patients with epilepsy for the first time in Iran.
Materials and Methods
The current cross sectional, correlational study was conducted on 211 patients with epilepsy referring to the Neurology Department and Comprehensive Epilepsy Center of Kashani Hospital in Isfahan, Iran from 2017 to 2018. Patients were selected through convenience sampling method and inclusion and exclusion criteria were used to enroll eligible subjects. Kashani Hospital in Isfahan was selected as the research setting because of ease of access to the study samples (simple or consecutive sampling). Diagnosis of epilepsy was confirmed by a epilepsy fellowship based on standard criteria [15] and psychological evaluations were performed by a psychiatric. The inclusion criteria were: having epilepsy and signing the written informed consent; at least six months of definitively being diagnosed with epilepsy and treatment onset; being able to answer the questions; no physical-psychological illnesses.
The exclusion criteria were: incidence of any acute diseases associated with seizure attacks during the data collection; no willingness to participate in the study; being missed to follow-up. The patients were enrolled if they met the inclusion criteria and had the desire for participation. The researchers referred to the study site and introduced themselves, explained the research objectives, provided explanations about the way to complete the questionnaires for patients and obtained the signed written consent forms from the ones who returned completed questionnaires. After obtaining permission from authorities, patients were placed in an appropriate place to complete the questionnaires.
The instrument used in the study was comprised of self-esteem and social support questionnaires and demographic characteristics checklist was also added to the first part. Demographic characteristics included age, gender, marital status, occupational status, educational level, and duration of the disease. The first questionnaire was the Rosenberg self-esteem scale. The content reliability and validity of the Rosenberg self-esteem scale was confirmed based on the comments of the developers and some preliminary studies [16].
The Rosenberg Self-Esteem Scale contains 10 general items that are scored based on a five-point Likert scale from 0 to 3 as: totally disagree (0), disagree (1), agree (2), and totally agree (3), the maximum score of the self-esteem questionnaire is 30. Scores above 25 indicate high self-esteem, 15-25 moderate self-esteem, and less than 15 indicate low self-esteem [17].
The second questionnaire was the social support questionnaire designed based on the Northouse Social Support Questionnaire (SSQ). The content reliability and validity of the SSQ was confirmed in another study [18]. The Northouse SSQ consists of 40 items in five dimensions as spouse, family members, friends, physician, and nurse. Each dimension has eight items that measure the level of social support perceived by patient’s spouse, family members, friends, physician, and nurse. The items are scored based on a five-point Likert scale from 1 to 5 as: totally disagree (1), disagree (2), no idea (3), agree (4), and totally agree (5).
The score of each dimension is separately calculated and the total score, which is calculated by summing the dimensions scores, ranges 40 to 200. The total score of perceived social support is interpreted as follows: low (40-92), moderate (93-146), and high (147-200), and the score of each dimension is also interpreted as: low (8-18), medium (19-29) and high (30-40). It should be noted that items of spouse dimension of are not omitted for single subjects. In addition, the Northouse SSQ has open-ended items to measure the social network of patients that was not applicable to the current study.
In the study, the collected data were analyzed using descriptive and statistical inference with SPSS V. 23. Descriptive statistics including frequency distribution, as well as mean and standard deviation was used to express data. Multiple regression analysis and Pearson Correlation Coefficient were also employed.
Results
In the present study, 211 patients with epilepsy referring to the Neurology Department and Comprehensive Epilepsy Center of Kashani Hospital were studied and all the participants completed questionnaires (100% response rate). Findings of the demographic variables are summarized in Table 1. The findings showed that 64.92% of the respondents were female and 35.1% male. Regarding the frequency distribution of respondents, in terms of age, the findings indicated that 10.4% of the respondents were within the age range of 20-25 years, 21.3% were 26-30 years, 33.1% were 31-35 years, 22.2% were 36-40 years , and 12.7% were above 41 years (Table 1).
Descriptive indices of the self-esteem score and the perceived social support score in each dimension are shown in Table 2. The findings revealed that the level of perceived social support was high in most of the studied cases and the highest score belonged to the family members’ dimension. The Pearson correlation showed no significant relationship between self-esteem and social support perceived by the spouse, family members, friends, physician, and nurse (P>0.05).
To investigate the prediction of self-esteem variable by perceived social support, the perceived social support components were introduced stepwise to self-esteem variables. Stepwise regression was evaluated and the results are shown on Table 3. All variables significantly retained themselves in five steps. The results of variance analysis showed that social support dimensions including spouse, family members, friends, physician, and nurse had a significant impact on self-esteem. The results of stepwise regression are reported in five steps. As shown in Table 4, the total score of perceived social support and self-esteem had a significant correlation (P<0.001).
Discussion
The current study aimed at investigating the relationship between perceived social support and self-esteem in patients with epilepsy referring to Kashani Hospital in Isfahan from 2017 to 2018. Descriptive findings revealed that the majority of the subjects were female patients (64.9%) and the age range of 26 to 30 years was predominant (33.1%). Results of the study indicated a significant correlation with 99% confidence interval between social support dimensions (including spouse, family members, friends, physician, and nurse) and self-esteem in the studied patients (P<0.001). Also, results of multiple regression analysis showed that spouse support, family members support, friends support, physician support, and nurse support predicted 12.4%, 41.5%, 4.6%, 4.7%, and 16.8% of self-esteem changes, respectively. These variables, in total, could predict about 80% of changes in self-esteem.
The results of the current study showed that most of the patients had high perceived social support. Family members are one of the most important elements of social support for patients, and the highest score among the dimensions of perceived social support belonged to the family members, which had the greatest impact on patients’ self-esteem. The family is the major source of social support for patients with epilepsy. To the best of authors’ knowledge, such findings might be attributed to Iranian culture, as the family members are the major
In a study on 160 patients treated in three different hemodialysis centers, Kara et al. reported the family as the major source of support for patients and suggested that perceived social support can affect the aspects non-adherence to dialysis diet and fluid restrictions [19]. Also, the results of studies demonstrate that social support in patients with heart failure can improve or maintain their quality of life. Janowski et al. found that patients with higher levels of perceived social support had a significantly higher quality of life, lower levels of depression, and higher acceptance of life with psoriasis. Song et al. also stated that social support is an important factor in self-care behaviors of patients with type II diabetes mellitus [20].
The results of the study showed that patients received the lowest level of social support from friends and this dimension had the lowest impact on patients’ self-esteem. One of the reasons for this finding can be the nature of the disease that affects patients’ communication skills. Other studies also showed that social support can improve the quality of life and reduce stress caused by hospitalization. In addition, perceived social support may reduce mortality in patients. In a study on patients undergoing hemodialysis, Welch et al. found that adherence to fluid restrictions was closely associated with social support in such patients [21]. The limitations of the current study were as follows: small sample size and not considering the impact of other social support aspects on self-esteem.
Conclusion
Social support can increase the self-esteem of patients with epilepsy. Increasing the self-esteem of such patients can help with their improvement (as an adjuvant). According to the results of the current study, patients perceived the least amount of social support from friends. One of the reasons for this finding could be the nature of the disease that affects patients’ communication skills. Also, further studies on the relation between social support and self-esteem in larger sample sizes are recommended.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by the Ethics Committee of Isfahan University of Medical Sciences (No. 397365). All the study procedures were in compliance with the ethical guidelines of the Declaration of Helsinki 1957.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
The authors contributions is as follows: Draft: Jafar Mehvari Habibabadi; Writing–review & editing: All authors; Funding acquisition: Jafar Mehvari Habibabadi; Resources: All authors; and Supervision: Jafar Mehvari Habibabadi and Maryam Izadi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
Authors hereby wish to thank the Comprehensive Epilepsy Center of Kashani Hospital, Isfahan, Iran.
References
- Ngugi AK, Bottomley C, Kleinschmidt I, Sander JW, Newton CR. Estimation of the burden of active and life‐time epilepsy: A meta‐analytic approach. Epilepsia. 2010; 51(5):883-90. [DOI:10.1111/j.1528-1167.2009.02481.x] [PMID] [PMCID]
- Unalan D, Soyuer F, Basturk M, Ersoy AO, Elmali F, Ozturk A. Perceived social support systems’ and depression’s effects on attitudes regarding coping strategies for the disease in patients with epilepsy. Neurosci. 2015; 20(1):17-26. [PMID] [PMCID]
- Epi4K Consortium, Epilepsy Phenome/Genome Project. De novo mutations in epileptic encephalopathies. Nature. 2013; 501(7466):217-21. [DOI:10.1038/nature12439] [PMID] [PMCID]
- Banerjee PN, Filippi D, Hauser WA. The descriptive epidemiology of epilepsy-A review. Epilepsy Res. 2009; 85(1):31-45. [DOI:10.1016/j.eplepsyres.2009.03.003] [PMID] [PMCID]
- Bruno E, Bartoloni A, Zammarchi L, Strohmeyer M, Bartalesi F, Bustos JA, et al. Epilepsy and neurocysticercosis in Latin America: A systematic review and meta-analysis. PLoS Negl Trop Dis. 2013; 7(10):e2480. [DOI:10.1371/journal.pntd.0002480] [PMID] [PMCID]
- Birbeck GL. Epilepsy care in developing countries: Part I of II. Epilepsy Curr. 2010; 10(4):75-9. [DOI:10.1111/j.1535-7511.2010.01362.x] [PMID] [PMCID]
- Rasolabadi M, Rasouli Ghahfarkhi SM, Ardalan M, Kalhor MM, Seidi J, Gharib A. Epilepsy research in Iran: A scientometric analysis of publications output during 2000-2014. Acta Inform Med. 2015; 23(6):374-8. [DOI:10.5455/aim.2015.23.374-378]
- Darabi L, Montazeri A, Ebrahimi F, Vahdaninia M, Togha M. [Clinical and demographic characteristics and quality of life in patients with epilepsy (Persian)]. Payesh. 2010; 9(2):215-21.
- Beals KP, Peplau LA, Gable SL. Stigma management and well-being: The role of perceived social support, emotional processing, and suppression. Pers Soc Psychol Bull. 2009; 35(7):867-79. [DOI:10.1177/0146167209334783] [PMID]
- Sheets RLJ, Mohr JJ. Perceived social support from friends and family and psychosocial functioning in bisexual young adult college students. J Couns Psychol. 2009; 56(1):152-63. [DOI:10.1037/0022-0167.56.1.152]
- Yadav S. Perceived social support, hope, and quality of life of persons living with HIV/AIDS: A case study from Nepal. Qual Life Res. 2010; 19(2):157-66. [DOI:10.1007/s11136-009-9574-z] [PMID]
- Charyton C, Elliott JO, Lu B, Moore JL. The impact of social support on health related quality of life in persons with epilepsy. Epilepsy Behav. 2009; 16(4):640-5. [DOI:10.1016/j.yebeh.2009.09.011] [PMID]
- Whatley A, DiIorio C, Yeager K. Examining the relationships of depressive symptoms, stigma, social support and regimen-specific support on quality of life in adult patients with epilepsy. Health Educ Res. 2010; 25(4):575-84. [DOI:10.1093/her/cyq001] [PMID] [PMCID]
- Paterson L, McKenzie K, Lindsay B. Stigma, social comparison and self‐esteem in adults with an intellectual disability. J Appl Res Intellect Disabil. 2012; 25(2):166-76. [DOI:10.1111/j.1468-3148.2011.00651.x] [PMID]
- Kerr M, Scheepers M, Arvio M, Beavis J, Brandt C, Brown S, et al. Consensus guidelines into the management of epilepsy in adults with an intellectual disability. J Intellect Disabil Res. 2009; 53(8):687-94. [DOI:10.1111/j.1365-2788.2009.01182.x] [PMID]
- Rajabi G, Bohlol N. [Validity and reliability of Rosenberg self-esteem scale in first year student of Shahid Chamran University (Persian)]. New Educ Approaches. 2006; 3(2):33-48.
- Mohammadi N, Sajadinegad MS. [The evaluation of psychometric properties of body image concern inventory and examination of a model about the rela-tionship between body mass index, body image dissatisfaction and self-esteem in adolescent girls (Persian)]. Q J Psychol Stud. 2006; 1(3):85-101.
- Broadhead W, Gehlbach SH, De Gruy FV, Kaplan BH. The Duke-UNC functional social support questionnaire: Measurement of social support in family medicine patients. Med Care. 1988; 26(7):709-23 [DOI:10.1097/00005650-198807000-00006] [PMID]
- Kara B, Caglar K, Kilic S. Nonadherence with diet and fluid restrictions and perceived social support in patients receiving hemodialysis. J Nurs Sch. 2007; 39(3):243-8. [DOI:10.1111/j.1547-5069.2007.00175.x] [PMID]
- Song Y, Song HJ, Han HR, Park SY, Nam S, Kim MT. Unmet needs for social support and effects on diabetes self-care activities in Korean Americans with type 2 diabetes. Diabetes Educ. 2012; 38(1):77-85. [DOI:10.1177/0145721711432456] [PMID] [PMCID]
- Welch JL, Thomas Hawkins C. Psycho-educational strategies to promote fluid adherence in adult hemodialysis patients: a review of intervention studies. Int J Nurs Stud. 2005; 42(5):597-608. [DOI:10.1016/j.ijnurstu.2004.09.015] [PMID]
Type of Study: Research |
Subject:
Special
Received: 2018/01/10 | Accepted: 2018/06/25 | Published: 2018/10/1
Received: 2018/01/10 | Accepted: 2018/06/25 | Published: 2018/10/1
References
1. Ngugi AK, Bottomley C, Kleinschmidt I, Sander JW, Newton CR. Estimation of the burden of active and life‐time epilepsy: A meta‐analytic approach. Epilepsia. 2010; 51(5):883-90. [DOI:10.1111/j.1528-1167.2009.02481.x] [PMID] [PMCID] [DOI:10.1111/j.1528-1167.2009.02481.x]
2. Unalan D, Soyuer F, Basturk M, Ersoy AO, Elmali F, Ozturk A. Perceived social support systems' and depression's effects on attitudes regarding coping strategies for the disease in patients with epilepsy. Neurosci. 2015; 20(1):17-26. [PMID] [PMCID]
3. Epi4K Consortium, Epilepsy Phenome/Genome Project. De novo mutations in epileptic encephalopathies. Nature. 2013; 501(7466):217-21. [DOI:10.1038/nature12439] [PMID] [PMCID] [DOI:10.1038/nature12439]
4. Banerjee PN, Filippi D, Hauser WA. The descriptive epidemiology of epilepsy-A review. Epilepsy Res. 2009; 85(1):31-45. [DOI:10.1016/j.eplepsyres.2009.03.003] [PMID] [PMCID] [DOI:10.1016/j.eplepsyres.2009.03.003]
5. Bruno E, Bartoloni A, Zammarchi L, Strohmeyer M, Bartalesi F, Bustos JA, et al. Epilepsy and neurocysticercosis in Latin America: A systematic review and meta-analysis. PLoS Negl Trop Dis. 2013; 7(10):e2480. [DOI:10.1371/journal.pntd.0002480] [PMID] [PMCID] [DOI:10.1371/journal.pntd.0002480]
6. Birbeck GL. Epilepsy care in developing countries: Part I of II. Epilepsy Curr. 2010; 10(4):75-9. [DOI:10.1111/j.1535-7511.2010.01362.x] [PMID] [PMCID] [DOI:10.1111/j.1535-7511.2010.01362.x]
7. Rasolabadi M, Rasouli Ghahfarkhi SM, Ardalan M, Kalhor MM, Seidi J, Gharib A. Epilepsy research in Iran: A scientometric analysis of publications output during 2000-2014. Acta Inform Med. 2015; 23(6):374-8. [DOI:10.5455/aim.2015.23.374-378] [DOI:10.5455/aim.2015.23.374-378]
8. Darabi L, Montazeri A, Ebrahimi F, Vahdaninia M, Togha M. [Clinical and demographic characteristics and quality of life in patients with epilepsy (Persian)]. Payesh. 2010; 9(2):215-21.
9. Beals KP, Peplau LA, Gable SL. Stigma management and well-being: The role of perceived social support, emotional processing, and suppression. Pers Soc Psychol Bull. 2009; 35(7):867-79. [DOI:10.1177/0146167209334783] [PMID] [DOI:10.1177/0146167209334783]
10. Sheets RLJ, Mohr JJ. Perceived social support from friends and family and psychosocial functioning in bisexual young adult college students. J Couns Psychol. 2009; 56(1):152-63. [DOI:10.1037/0022-0167.56.1.152] [DOI:10.1037/0022-0167.56.1.152]
11. Yadav S. Perceived social support, hope, and quality of life of persons living with HIV/AIDS: A case study from Nepal. Qual Life Res. 2010; 19(2):157-66. [DOI:10.1007/s11136-009-9574-z] [PMID] [DOI:10.1007/s11136-009-9574-z]
12. Charyton C, Elliott JO, Lu B, Moore JL. The impact of social support on health related quality of life in persons with epilepsy. Epilepsy Behav. 2009; 16(4):640-5. [DOI:10.1016/j.yebeh.2009.09.011] [PMID] [DOI:10.1016/j.yebeh.2009.09.011]
13. Whatley A, DiIorio C, Yeager K. Examining the relationships of depressive symptoms, stigma, social support and regimen-specific support on quality of life in adult patients with epilepsy. Health Educ Res. 2010; 25(4):575-84. [DOI:10.1093/her/cyq001] [PMID] [PMCID] [DOI:10.1093/her/cyq001]
14. Paterson L, McKenzie K, Lindsay B. Stigma, social comparison and self‐esteem in adults with an intellectual disability. J Appl Res Intellect Disabil. 2012; 25(2):166-76. [DOI:10.1111/j.1468-3148.2011.00651.x] [PMID] [DOI:10.1111/j.1468-3148.2011.00651.x]
15. Kerr M, Scheepers M, Arvio M, Beavis J, Brandt C, Brown S, et al. Consensus guidelines into the management of epilepsy in adults with an intellectual disability. J Intellect Disabil Res. 2009; 53(8):687-94. [DOI:10.1111/j.1365-2788.2009.01182.x] [PMID] [DOI:10.1111/j.1365-2788.2009.01182.x]
16. Rajabi G, Bohlol N. [Validity and reliability of Rosenberg self-esteem scale in first year student of Shahid Chamran University (Persian)]. New Educ Approaches. 2006; 3(2):33-48.
17. Mohammadi N, Sajadinegad MS. [The evaluation of psychometric properties of body image concern inventory and examination of a model about the rela-tionship between body mass index, body image dissatisfaction and self-esteem in adolescent girls (Persian)]. Q J Psychol Stud. 2006; 1(3):85-101.
18. Broadhead W, Gehlbach SH, De Gruy FV, Kaplan BH. The Duke-UNC functional social support questionnaire: Measurement of social support in family medicine patients. Med Care. 1988; 26(7):709-23 [DOI:10.1097/00005650-198807000-00006] [PMID] [DOI:10.1097/00005650-198807000-00006]
19. Kara B, Caglar K, Kilic S. Nonadherence with diet and fluid restrictions and perceived social support in patients receiving hemodialysis. J Nurs Sch. 2007; 39(3):243-8. [DOI:10.1111/j.1547-5069.2007.00175.x] [PMID] [DOI:10.1111/j.1547-5069.2007.00175.x]
20. Song Y, Song HJ, Han HR, Park SY, Nam S, Kim MT. Unmet needs for social support and effects on diabetes self-care activities in Korean Americans with type 2 diabetes. Diabetes Educ. 2012; 38(1):77-85. [DOI:10.1177/0145721711432456] [PMID] [PMCID] [DOI:10.1177/0145721711432456]
21. Welch JL, Thomas Hawkins C. Psycho-educational strategies to promote fluid adherence in adult hemodialysis patients: a review of intervention studies. Int J Nurs Stud. 2005; 42(5):597-608. [DOI:10.1016/j.ijnurstu.2004.09.015] [PMID] [DOI:10.1016/j.ijnurstu.2004.09.015]
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
