Mon, May 6, 2024
Volume 3, Issue 4 (Autumn 2017)
Caspian J Neurol Sci 2017, 3(4): 175-184 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Amir F, Ahadi H, Nikkhah K, Seirafi M. The Effectiveness of Acceptance and Commitment Group Therapy and Group Logotherapy in Reducing Perceived Stress among MS Patients. Caspian J Neurol Sci 2017; 3 (4) :175-184
URL: http://cjns.gums.ac.ir/article-1-193-en.html
URL: http://cjns.gums.ac.ir/article-1-193-en.html


1- Department of Psychology, Islamic Azad University, Kish Branch, Kish, Iran
2- Professor of Psychology, Department of Psychology, Islamic Azad University, Karaj Branch, Karaj, Iran; drhahadi5@gmail.com
3- Professor of Neurology, Department of Neurology, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
4- Assistant Professor of Psychology, Department of Psychology, Islamic Azad University, Karaj Branch, Karaj, Iran
2- Professor of Psychology, Department of Psychology, Islamic Azad University, Karaj Branch, Karaj, Iran; drhahadi5@gmail.com
3- Professor of Neurology, Department of Neurology, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
4- Assistant Professor of Psychology, Department of Psychology, Islamic Azad University, Karaj Branch, Karaj, Iran
Full-Text [PDF 785 kb]
(1814 Downloads)
| Abstract (HTML) (5508 Views)

Full-Text: (2211 Views)
Introduction
ultiple sclerosis (MS) is a chronic incurable disease of the central nervous system in which myelin sheath is progressively destroyed (1).
Approximately 1 per 1000 people suffers from MS which has the global prevalence rate of about 1.1 million (2). Based on the report by Iran MS Society, there are around 40,000 MS patients in this country, 9000 of whom are registered (3). Studies show that the most frequent age of onset is 20-40 years and that MS is 1.5-3 times more prevalent among women than among men (4). It adversely affects daily performance, social and family life, independence, and future plans,
subjecting the patients and their families to extreme stress. Moreover, approximately 80% of MS patients suffer from varying degrees of disability. Only 1 in every 5 patients has a stable state without progression towards disability (5).
According to research, in addition to physical symptoms, MS patients experience much higher levels of mental disorders, e.g. anxiety and stress, compared to healthy individuals. Beiske et al. (2008) found that patients in the initial stages of MS exhibited higher anxiety and depression levels (6).
Additionally, these patients report that psychological stress aggravates disease symptoms (7). A number of studies indicate that prolonged exposure to a wide range of stressful events exacerbates MS symptoms. Furthermore, MRI observations suggest that stress affects brain systems in these patients (8). Results of meta-analyses also demonstrate the significant relationship between stressful events and symptom exacerbation (9). According to studies, repeated stressful events decrease the performance of the physiological stress response in MS patients and prevent their bodies from effectively responding to stress, leading to more physical and mental symptoms (10). Considering various problems (e.g.exacerbated disease symptoms and increased costs and mortality rates) caused by stress for MS patients (11), it is essential to pay attention to and reduce stress in them. Due to numerous adverse effects of pharmacotherapy, it seems to be logical to use non-pharmacological approaches in order to decrease anxiety and stress in MS patients. As a result, non-pharmacological approaches- including group therapies - have attracted considerable attention from all patients, including MS patients, in recent years. Use of group therapy, alone or combined with other treatments, has significantly increased in recent years. By targeting social interactions, this method assists group members in garnering insight into their social behavior, gaining new experiences, enjoying social support, and acting more successfully in their interaction with others. All these enhance their self confidence and self-efficacy (12). Acceptance and commitment therapy (ACT) is a group therapy which has recently
received considerable attention from researchers (13). ACT is based on relational systems theory which views stress avoidance as the patients’ main problem, leading to disability and decreased life satisfaction. Based on this theory, avoidance occurs when negative thoughts and emotions have
excessive and harmful effects on behaviors. Consequently, the main treatment method in ACT is confronting the patients with situations they used to avoid (14). Contrary to other treatments (including CBT) which focus on decreasing or controlling the symptoms, ACT aims to enhance the acceptance of negative reactions
(thoughts, emotions, and bodily sensations) to help the patients engage in meaningful activities which cannot be directly changed,regardless of how much pain or stress it may result in. ACT aims to promote the patients’functioning by enhancing mental flexibility(13). Many treatments help patients have a better feeling. They attempt to make patients feel better emotionally and experience fewer symptoms by the end of the treatment period.
Nevertheless, ACT focuses on a better life,regardless of a better feeling (15). Focusing on two major treatment processes in ACT, i.e.acceptance and values-based action, Vowles et al. (2011) indicated that the patients had animproved physical and emotional functioning compared to the beginning of treatment as well as good maintenance of treatment achievements compared to an earlier followup assessment (16).
Another group therapy which can affect MS symptoms is group logotherapy. This method is an existential approach which creates a structure of meaningfulness to help patients who struggle with finding meaning in their lives (17). What matters in logotherapy is the confirmation of unique human potentials. Having meaning in life is an important factor in mental health, associated with many psychological components (18).According to Frankl, hopeless, depressed, and anxious people as well as those who experience loneliness usually complain of the lack of meaning or aim in their lives. Nothing commits them to life or is of value to them.
Logotherapy is a philosophical approach towards people and their existence. It deals with important themes and concepts such as the meaning of pain, existential vacuum, life and death, freedom, responsibility towards self and others, search for meaning, and coping with meaninglessness. This approach forces people to see beyond life’s daily events and problems (19). The literature suggests the effectiveness of psychological interventions based on logotherapy in the improvement of mental and physical states of patients suffering from chronic diseases, including MS (20,21). Numerous psychological and social factors affect stress in MS patients,namely, mental obsessions as a result of the disease as well as fear of death and worrying about the future, losing one’s job, and treatment costs. If patients receive help in strengthening hope and meaning in their lives,it is assumed that their self-confidence and ability to deal with issues would be enhanced (22). Overall, it is clear that group therapies such as ACT and logotherapy are effective interventions in reducing stress among MS patients. So far, however, little relevant research has been conducted. As stress causes numerous problems for these patients, the use of these methods appears logical. Therefore,the present study was conducted to examine the effectiveness of group therapy (ACT and logotherapy) in reducing perceived stress among MS patients. Research hypotheses/questions were as follows: 1. Acceptance and commitment group therapy decreases perceived stress among MS patients. 2. Group logotherapy decreases perceived stress among MS patients. 3. Do acceptance and commitment group therapy and group logotherapy significantly differ in terms of their effects on perceived stress among MS patients?
Materials and Methods
This research was a pretest-posttest controlled quasi-experimental study. Research population was comprised of all (n=3000) MS patients who were members of Mashhad MS Society, Iran. Using convenience sampling,33 patients who met the inclusion criteria(age: 20-40 years old; not receiving ACT or treatment for stress and hopelessness; the ability to talk; and not permanently wheelchair-bound) were selected as the initial sample and completed Cohen et al.'s Perceived Stress Scale (PSS). The lowest and highest scores on this scale are 0 and 56,respectively. The final sample was collected from among those who had scored above 45 on PSS. The subjects were matched based on pre-test scores and demographic characteristics (sex, education level, marital status, and duration of disease) and divided into three groups of 11 (ACT, logotherapy, and control). The protocol of ACT group therapy sessions was based on Hayes,Strosahl, and Wilson (1999) and comprised twelve 90-minute sessions three times a week.Group logotherapy included eight 90-minute sessions in four consecutive weeks within the treatment framework described by Hutzell (2002). The control group received no intervention. At the end of the treatment period, PSS was once more administered to all the groups.
Instruments:
Instruments included a researcher-made questionnaire for evaluating personal characteristics (age, marital status, incomelevel, education level, and history of physical and mental symptoms) as well as the Persian version of 14-item Perceived Stress Scale(PSS-14) for evaluating the components of perceived stress. PSS, designed by Cohen et al. (1983), has 3-, 10-, and 14-item versions.It is used for measuring perceived general stress in the past month and evaluates thoughts and emotions regarding stressful events, control, dominance, and coping with mental pressure and perceived stress. PSS also examines the risk factors of behavioral disorders and shows the process of stressful relationships. Cronbach’s alpha was reported 84%-85% for PSS in three studies (25),showing its reliability. Salehi Ghadri (1994) reported the Cronbach’s alpha of 75%; the validity of this questionnaire was also confirmed by a simple correlation coefficient of 0.63 (p<0.05) (26). Sepahvand et al. (2009) reported the Cronbach’s alpha of 80% for this scale (27). PSS is scored on a five-point Likert scale (Never = 0; Almost never = 1;Sometimes = 2; Fairly often = 3; Very often =4). Responses to questions 4, 5, 6, 7, 9, 10,and 13 are reversed (from Never = 4 to Very often = 0). Final scores range from 0 to 56,with higher scores indicating higher levels of perceived stress.The frequency of qualitative and the mean and standard deviation (SD) of quantitative factors were determined. And the One-way ANCOVA was used for analysis of data in SPSS software version 20.
Results
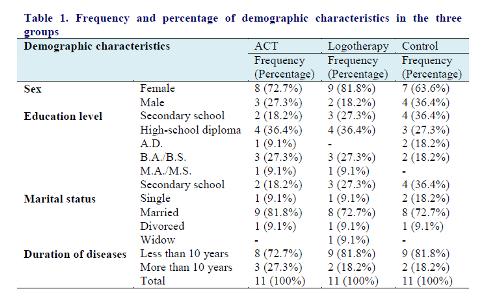
In this study, 33 MS patients were divided into three experimental groups and one control group. An attempt was made to match the groups in terms of demographic characteristics (sex, education level, marital status and duration of disease). Mean age was 36.45 years in the ACT group, 34.81 years in the logotherapy group, and 36.27 years in the control group. Table 1 presents the frequency and percentage of demographic characteristics (sex, education level, marital status, and duration of disease). Downloaded from
ultiple sclerosis (MS) is a chronic incurable disease of the central nervous system in which myelin sheath is progressively destroyed (1).
Approximately 1 per 1000 people suffers from MS which has the global prevalence rate of about 1.1 million (2). Based on the report by Iran MS Society, there are around 40,000 MS patients in this country, 9000 of whom are registered (3). Studies show that the most frequent age of onset is 20-40 years and that MS is 1.5-3 times more prevalent among women than among men (4). It adversely affects daily performance, social and family life, independence, and future plans,
subjecting the patients and their families to extreme stress. Moreover, approximately 80% of MS patients suffer from varying degrees of disability. Only 1 in every 5 patients has a stable state without progression towards disability (5).
According to research, in addition to physical symptoms, MS patients experience much higher levels of mental disorders, e.g. anxiety and stress, compared to healthy individuals. Beiske et al. (2008) found that patients in the initial stages of MS exhibited higher anxiety and depression levels (6).
Additionally, these patients report that psychological stress aggravates disease symptoms (7). A number of studies indicate that prolonged exposure to a wide range of stressful events exacerbates MS symptoms. Furthermore, MRI observations suggest that stress affects brain systems in these patients (8). Results of meta-analyses also demonstrate the significant relationship between stressful events and symptom exacerbation (9). According to studies, repeated stressful events decrease the performance of the physiological stress response in MS patients and prevent their bodies from effectively responding to stress, leading to more physical and mental symptoms (10). Considering various problems (e.g.exacerbated disease symptoms and increased costs and mortality rates) caused by stress for MS patients (11), it is essential to pay attention to and reduce stress in them. Due to numerous adverse effects of pharmacotherapy, it seems to be logical to use non-pharmacological approaches in order to decrease anxiety and stress in MS patients. As a result, non-pharmacological approaches- including group therapies - have attracted considerable attention from all patients, including MS patients, in recent years. Use of group therapy, alone or combined with other treatments, has significantly increased in recent years. By targeting social interactions, this method assists group members in garnering insight into their social behavior, gaining new experiences, enjoying social support, and acting more successfully in their interaction with others. All these enhance their self confidence and self-efficacy (12). Acceptance and commitment therapy (ACT) is a group therapy which has recently
received considerable attention from researchers (13). ACT is based on relational systems theory which views stress avoidance as the patients’ main problem, leading to disability and decreased life satisfaction. Based on this theory, avoidance occurs when negative thoughts and emotions have
excessive and harmful effects on behaviors. Consequently, the main treatment method in ACT is confronting the patients with situations they used to avoid (14). Contrary to other treatments (including CBT) which focus on decreasing or controlling the symptoms, ACT aims to enhance the acceptance of negative reactions
(thoughts, emotions, and bodily sensations) to help the patients engage in meaningful activities which cannot be directly changed,regardless of how much pain or stress it may result in. ACT aims to promote the patients’functioning by enhancing mental flexibility(13). Many treatments help patients have a better feeling. They attempt to make patients feel better emotionally and experience fewer symptoms by the end of the treatment period.
Nevertheless, ACT focuses on a better life,regardless of a better feeling (15). Focusing on two major treatment processes in ACT, i.e.acceptance and values-based action, Vowles et al. (2011) indicated that the patients had animproved physical and emotional functioning compared to the beginning of treatment as well as good maintenance of treatment achievements compared to an earlier followup assessment (16).
Another group therapy which can affect MS symptoms is group logotherapy. This method is an existential approach which creates a structure of meaningfulness to help patients who struggle with finding meaning in their lives (17). What matters in logotherapy is the confirmation of unique human potentials. Having meaning in life is an important factor in mental health, associated with many psychological components (18).According to Frankl, hopeless, depressed, and anxious people as well as those who experience loneliness usually complain of the lack of meaning or aim in their lives. Nothing commits them to life or is of value to them.
Logotherapy is a philosophical approach towards people and their existence. It deals with important themes and concepts such as the meaning of pain, existential vacuum, life and death, freedom, responsibility towards self and others, search for meaning, and coping with meaninglessness. This approach forces people to see beyond life’s daily events and problems (19). The literature suggests the effectiveness of psychological interventions based on logotherapy in the improvement of mental and physical states of patients suffering from chronic diseases, including MS (20,21). Numerous psychological and social factors affect stress in MS patients,namely, mental obsessions as a result of the disease as well as fear of death and worrying about the future, losing one’s job, and treatment costs. If patients receive help in strengthening hope and meaning in their lives,it is assumed that their self-confidence and ability to deal with issues would be enhanced (22). Overall, it is clear that group therapies such as ACT and logotherapy are effective interventions in reducing stress among MS patients. So far, however, little relevant research has been conducted. As stress causes numerous problems for these patients, the use of these methods appears logical. Therefore,the present study was conducted to examine the effectiveness of group therapy (ACT and logotherapy) in reducing perceived stress among MS patients. Research hypotheses/questions were as follows: 1. Acceptance and commitment group therapy decreases perceived stress among MS patients. 2. Group logotherapy decreases perceived stress among MS patients. 3. Do acceptance and commitment group therapy and group logotherapy significantly differ in terms of their effects on perceived stress among MS patients?
Materials and Methods
This research was a pretest-posttest controlled quasi-experimental study. Research population was comprised of all (n=3000) MS patients who were members of Mashhad MS Society, Iran. Using convenience sampling,33 patients who met the inclusion criteria(age: 20-40 years old; not receiving ACT or treatment for stress and hopelessness; the ability to talk; and not permanently wheelchair-bound) were selected as the initial sample and completed Cohen et al.'s Perceived Stress Scale (PSS). The lowest and highest scores on this scale are 0 and 56,respectively. The final sample was collected from among those who had scored above 45 on PSS. The subjects were matched based on pre-test scores and demographic characteristics (sex, education level, marital status, and duration of disease) and divided into three groups of 11 (ACT, logotherapy, and control). The protocol of ACT group therapy sessions was based on Hayes,Strosahl, and Wilson (1999) and comprised twelve 90-minute sessions three times a week.Group logotherapy included eight 90-minute sessions in four consecutive weeks within the treatment framework described by Hutzell (2002). The control group received no intervention. At the end of the treatment period, PSS was once more administered to all the groups.
Instruments:
Instruments included a researcher-made questionnaire for evaluating personal characteristics (age, marital status, incomelevel, education level, and history of physical and mental symptoms) as well as the Persian version of 14-item Perceived Stress Scale(PSS-14) for evaluating the components of perceived stress. PSS, designed by Cohen et al. (1983), has 3-, 10-, and 14-item versions.It is used for measuring perceived general stress in the past month and evaluates thoughts and emotions regarding stressful events, control, dominance, and coping with mental pressure and perceived stress. PSS also examines the risk factors of behavioral disorders and shows the process of stressful relationships. Cronbach’s alpha was reported 84%-85% for PSS in three studies (25),showing its reliability. Salehi Ghadri (1994) reported the Cronbach’s alpha of 75%; the validity of this questionnaire was also confirmed by a simple correlation coefficient of 0.63 (p<0.05) (26). Sepahvand et al. (2009) reported the Cronbach’s alpha of 80% for this scale (27). PSS is scored on a five-point Likert scale (Never = 0; Almost never = 1;Sometimes = 2; Fairly often = 3; Very often =4). Responses to questions 4, 5, 6, 7, 9, 10,and 13 are reversed (from Never = 4 to Very often = 0). Final scores range from 0 to 56,with higher scores indicating higher levels of perceived stress.The frequency of qualitative and the mean and standard deviation (SD) of quantitative factors were determined. And the One-way ANCOVA was used for analysis of data in SPSS software version 20.
Results
In this study, 33 MS patients were divided into three experimental groups and one control group. An attempt was made to match the groups in terms of demographic characteristics (sex, education level, marital status and duration of disease). Mean age was 36.45 years in the ACT group, 34.81 years in the logotherapy group, and 36.27 years in the control group. Table 1 presents the frequency and percentage of demographic characteristics (sex, education level, marital status, and duration of disease). Downloaded from

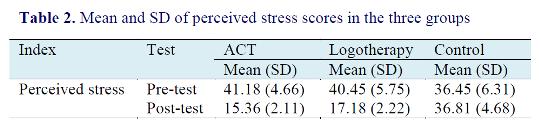
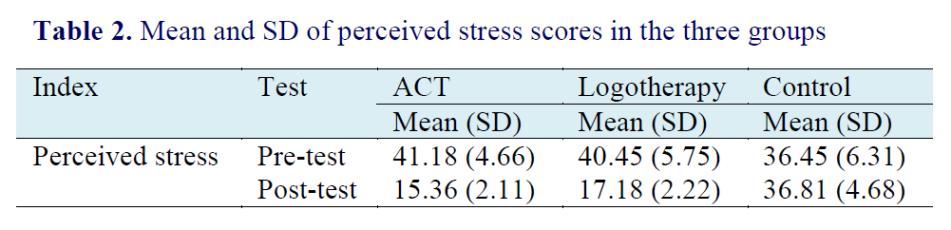
Table 2 shows the mean and standard deviation (SD) of perceived stress in the three groups on pre- and post-tests.
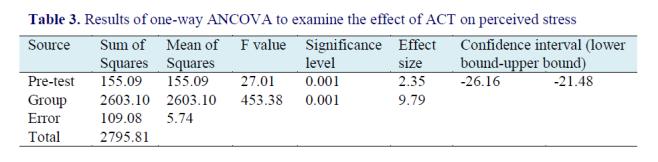
One-way ANCOVA was employed to explore the effect of ACT on perceived stress.In this analysis, group (ACT vs. control) (between-subject factor), the subjects’ scores on PSS on pre-test (as the control variable), and their scores on post-test (as the dependent variable) entered the model. Results are shown in table 3.
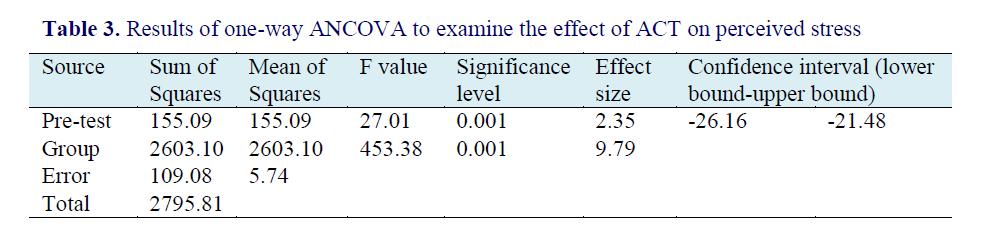
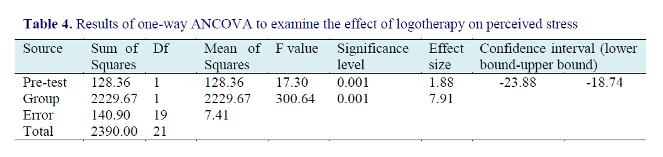
Prior to performing one-way ANCOVA,the normality of PSS scores was checked using Levene's test based on the assumption of equal variances for the scores. Results of Levene’s test revealed that the assumption of equal variances holds (F=0.33, p>0.05). Therefore, the assumptions of one-way ANCOVA hold and can thus be used. Results of one-way ANCOVA (table 3) indicate that the effect of pre-test scores was significant (F=27.01, p<0.001). This means that there was a significant relationship between PSS pre- and post-test scores. Moreover, the above table suggests that, after controlling for pre-test scores, the effect of group on PSS posttest scores was significant (F=453.38,p<0.001). In other words, there was a significant difference between ACT group and the control group in terms of mean PSS post-test scores. Based on descriptive indices (table 2), mean PSS post-test score of the ACT group (15.36) was significantly lower than that of the control group (36.81). Thus,the first hypothesis is confirmed, i.e. ACT significantly reduces perceived stress in MS patients. To further investigate the difference among groups, effect size (Cohen’s d) was also calculated. According to Cohen, effect sizes up to 0.2 are small, up to 0.5 is average, and above 0.8 are large (Becker, 2000). Based on Table 3, the effect size for the effect of group on perceived stress was more than 0.8 (9.79). This means that the difference between ACT group and the control group was very large in terms of perceived stress.One-way ANCOVA was employed to check the effect of group logotherapy on perceived stress. In this analysis, group(logotherapy vs. control) (as between-subject factor), the subjects’ scores on PSS on pretest (as the control variable), and their scores on post-test (as the dependent variable)entered the model. Results are demonstrated in table 4.
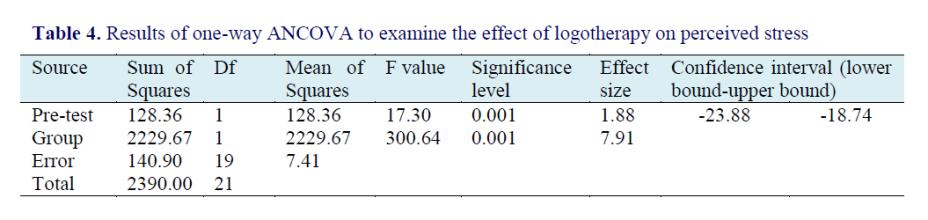
Prior to conducting one-way ANCOVA, the assumption of homogeneous variance between the groups was checked using Levene's test on perceived stress scores. Results of Levene’s test suggested that the assumption of equal variances holds (F=0.08,p>0.05). Therefore, the assumptions of oneway ANCOVA hold and can thus be used.Results of one-way ANCOVA (table 4) indicate that the effect of pre-test scores was significant (F=17.30, p<0.001). This means that there was a significant relationship between PSS pre- and post-test scores.Moreover, the above table suggests that, after controlling for pre-test scores, the effect ofgroup on PSS post-test scores was significant (F=300.64, p<0.001). In other words, there was a significant difference between logotherapy and control groups n terms of mean PSS post-test scores. Based on descriptive indices (table 2), mean PSS posttest score of the logotherapy group (17.18) was significantly lower than that of the control group (36.81). Thus, the second hypothesis is confirmed, i.e. logotherapy significantly decreases perceived stress in MS patients. Based on Table 4, the effect size for the effect of group on perceived stress was more than 0.8 (7.91). This means that the difference between logotherapy and control groups was very large in terms of perceived stress. Furthermore, one-way ANCOVA was incorporated to check the difference between ACT and logotherapy groups in terms of reducing perceived stress among MS patients. In this analysis, group (ACT vs. logotherapy) (as the between-subject factor), the subjects’ scores on PSS on pre-test (as the control variable), and their scores on post-test (as the dependent variable) entered the model.Results are hown in table 5

Prior to performing one-way ANCOVA,the assumption of homogenous variance between the groups was checked using Levene's test on perceived stress scores.Results of Levene’s test suggested that the assumption of equal variances holds (F=0.07, p>0.05). Therefore, the assumptions of oneway ANCOVA hold and it can thus be used. Results of one-way ANCOVA (table 5) indicate that the effect of pre-test scores was not significant (F=1.83, p<0.05). This means that there was no significant relationship between PSS pre- and post-test scores.Moreover, the above table suggests that, after controlling for pre-test scores, the effect of group on PSS post-test scores was significant (F=4.40, p<0.05). In other words, there was a significant difference between ACT and logotherapy groups in terms of mean PSS post-test scores. Based on descriptive indices (table 2), mean PSS post-test score of the ACT group (15.36) was significantly lower than that of the logotherapy group (17.18). These results indicate a positive answer to the research question. Based on Table 5, the effect size for the effect of group on perceived stress was more than 0.8 (0.93). This means that the difference between ACT and logotherapy groups was large in terms of perceived stress.
Discussion
The present study aimed to compare the effectiveness of acceptance and commitment group therapy and group logotherapy in reducing perceived stress among MS patients. Based on the results, both therapies were effective in reducing perceived stress among MS patients, i.e. both groups had a lower perceived stress than the control group following the interventions. Results also showed that ACT had a greater effect than logotherapy on reducing perceived stress among these patients. In line with the present study, a number of studies suggest that ACT can improve MS symptoms (28,29,30,31). ACT may have the effect by changing the patients’ attitude in the first sessions. In addition, ACT works by creating and developing “acceptance” and “enhancing value-based action” in patients (32). Contrary to other therapies, ACT imposes no specific value or lifestyle on patients. Here, patients decide to change based on their own value system. Attention to committed action is another process highlighted in this treatment protocol for MS patients. Encouraging patients to clarify values, determine goals, predict obstacles and, in the end, commit to actions for achieving those goals based on values despite the disease, saves the patients from repetitive negative thoughts and feelings, helps them realize their goals, and leads to happiness, thereby reduce stress (33). Results also revealed that group logotherapy successfully educed perceived stress in these patients. This finding is consistent with numerous studies showing the effectiveness of logotherapy in patients’ and healthy individuals’ physical and mental health (34,35,36,37). Setting goals and finding meaning of life can help MS patients overcoming symptoms such as anxiety, stress, and hopelessness (18), as hopelessness exacerbates symptoms and increases stress in them. Therefore, psychological interventions which aim to promote hope, meaning, and goals in life can be useful for this group (38). Furthermore, finding meaning reduces psychological pressures and the negative outcomes of the disease, thereby enhances mental health and adjustment. Logotherapy helps patients to stop focusing on what has been lost and, instead, search for meaning despite hopelessness. Thus, according to logotherapy, life always has meaning, and these patients can cope better under stressful situations. What matters in logotherapy is the confirmation of unique human potentials which can turn tragedies into personal victories and change unpleasant situations into pleasant ones (39). Frankl believes that,in the face of unchangeable situations such as an incurable disease, people have the opportunity to find the deepest and greatest meaning of life and thus cope with stressful and unpleasant conditions (40). These results can have important clinical implications for MS patients; the use of complementary psychological therapies together with pharmacotherapy can be more effective for patients while decreasing the costs of treatment. Moreover, the use of ACT group therapy and group logotherapy can enhance their ability to cope with unpleasant conditions and stresses caused during the course of the disease, thereby creating a better condition for them. Another result of the present study was the further effectiveness of ACT compared to logotherapy in reducing perceived stress among MS patients. The use of more behavioral and performance exercises in ACT may have resulted in its superiority. Although group logotherapy had significant effects, better results may be achieved using behavioral exercises and encouraging MS patients to utilize performance techniques.
Conclusion
The present study had certain limitations,including the lack of total control over variables such as environmental, personal, familial, psychological, and physical factors (e.g. issues related to disease relapse and medications), a number of which were, nevertheless, identified and controlled by the researchers. Moreover, limiting the population to those who were members of Iran MS Society may limit the generalizability of results to other patients. In addition, due to the adverse physical and psychological conditions of a large number of patients as well as problems which could arise as a result of their participation, the researchers had to assign a small number of subjects to each group. We recommend that future studies recruit MS patients who are not members of Iran MS Society. Also, based on the effectiveness of ACT group therapy and logotherapy in reducing perceived stress, we suggest that experts include these methods in their treatments Conflict of Interest The authors have no conflict of interest.
References
1. Halper J, Holland NJ. Multiple Sclerosis: A Self-Care Guide to Wellness. Demos Medical Publishing; 2005.
2. Mitchell AJ, Benito-León J, González JM, Rivera-Navarro J. Quality of Life and Its Assessment in Multiple Sclerosis: Integrating Physical and Psychological Components of Wellbeing. Lancet Neurol 2005;4(9):556-66.
3. Aleyasin H, Sarai A, Alaeddini F,Ansarian E, Lotfi J, Sanati MH. Multiple Sclerosis: a Study of 318 Cases. Arch Tran Med 2012; 5:249.
4. MCcabe MP. Mood and Self-esteem of Persons with Multiple Sclerosis Following an Exacerbation. J Psychosom Res 2005;59(3):161-6.
5. Ghafari S, Ahmadi F, Nabavi SM, Memarian R. Effect of Progressive Muscle Relaxation on Depression, Anxiety and Stress in Patients with MS. Res Med J Shahid Beheshti Uni Med Sci Health 2008;32: 45-53. [Text in Persian].
6. Beiske AG, Svensson E, Sandanger I, Czujko B, Pederson ED, Aarseth JH, et al. Depression and Anxiety amongst Multiple Sclerosis Patients. Eur J Neurol 2008; 15(3):239-45.
7. Yamout B, Itani S, Hourany R, Sibaii AM,Yaghi S. The Effect of War Stress on Multiple Sclerosis Exacerbations and Radiological Disease Activity. J Neurol Sci 2010;288(1- 2):42-4.
8. Mohr DC, Goodkin DE, Bacchetti P,Boudewyn AC, Huang L, Marrietta P, et al. Psychological Stress and the Subsequent Appearance of New Brain MRI Lesions in MS. Neurology2000;55(1):55-61
9. Heesen C, Mohr DC, Huitinga I, Bergh FT, Gaab J, Otte C, et al. Stress Regulation in Multiple Sclerosis Current Issues and Concepts. Mult Scler 2007;13(2):143-8.
10. Gold SM, Mohr DC, Huitinga I, Flachenecker P, Sternberg EM, Heesen C. The Role of Stress-response Systems for the Pathogenesis and Progression of MS. Trends Immunol 2005;26(12):644-52.
11. Esmonde L, Long AF. Complementary Therapy Use by Persons with Multiple Sclerosis: Benefits and Research Priorities. Complement Ther Clin Pract 2008; 14(3): 176- 84.
12. Crawford JD, McIvor GP. Group Psychotherapy: Benefits in Multiple Sclerosis. Arch Phys Med Rehabil 1985; 66: 810-3.
13. Prevedini AB, Presti G, Rabitti E, Miselli G, Moderato P. Acceptance and Commitment Therapy (ACT): the Foundation of the Therapeutic Model and an Overview of Its Contribution to the Treatment of Patients with Chronic Physical Diseases. G Ital Med Lav Ergon. 2011;33(1): A53-63.
14. Villatte JL, Vilardaga R, Villatte M, Vilardaga JC, Atkins DC, Hayes SC. Acceptance and Commitment Therapy Modules: Differential Impact on Treatment Processes and Outcomes. Behav Res Ther 2016; 77:52-61.
15. Hiratzka J, Rastegar F, Contag AG, Norvell DC, Anderson PA, Hart RA. Adverse Event Recording and Reporting in Clinical Trials Comparing Lumbar Disk Replacement with Lumbar Fusion: A Systematic Review. Global Spine J 2015;5(06):486-95.
16. Vowles KE, McCracken LM, O’Brien JZ. Acceptance and Values-based Action in Chronic Pain: a Three-year Follow-up Analysis of Treatment Effectiveness and Process. Behav Res Ter 2011;49(11):748-55.
17. Yalom ID, Leszcz M. Theory and Practice of Group Psychotherapy. Basic books; 2005.
18. Kang K, Im J, Kim H, Kim S, Song M, Sim S. The Effect of Logotherapy on the Suffering, Finding Meaning, and Spiritual Well-being of Adolescents with Terminal Cancer. Child Health Nurs Res 2009;15(2):136-44.
19. Robatmili S, Sohrabi F, Shahrak MA,Talepasand S, Nokani M, Hasani M. The Effect of Group Logotherapy on Meaning in Life and Depression Levels of Iranian Students. Int J Adv Couns 2015;37(1):54-62.
20. Bruce JM, Lynch SG. Personality Traits in Multiple Sclerosis: Association with Mood and Anxiety Disorders. J Psychosom Res 2011;70(5):479-85.
21. Burns MN, Siddique J, Fokuo JK, Mohr DC. Comorbid Anxiety Disorders and Treatment of Depression in People with Multiple Sclerosis.
22. Way SW, Popko B. Harnessing the Integrated
Stress Response for the Treatment of Multiple
Sclerosis. Lancet Neurol 2016;15(4):434-43.
23. Hayes SC, Strosahl KD, Wilson KG.
Acceptance and Commitment Therapy: An
Experiential Approach to Behavior Change.
Guilford Press; 1999.
24. Hutzell RR. A General Course of Group
Analysis. Viktor Frankl Foundation of South
Africa 2002;7:15-26.
25. Cohen S, Kamarck T. Mermelstein R. Global
Measure of Perceived Stress. Journal of Health
and Social Behavior 1983;24(4):385-96.
26. Salehi Ghadri J. Efficacy of Multiplicity of
Roles and Satisfaction with It on the Self
Esteem and Stress in Female Teachers. MA
Thesis, Tarbiat Modares University, 1994.
[Text in Persian]
27. Sepahvand T, Gilani B, Zamani R. The
Relationship between Explanatory Styles with
Perceived Stress and General Health. Journal
of Psychology and Education 2009; 38(4):27-
43. [Text in Persian]
28. Nordin L, Rorsman I. Cognitive Behavioural
Therapy in Multiple Sclerosis: a Randomized
Controlled Pilot Study of Acceptance and
Commitment Therapy. J Rehabil Med
2012;44(1):87-90.
29. Sheppard SC, Forsyth JP, Hickling EJ, Bianchi
J. A Novel Application of Acceptance and
Commitment Therapy for Psychosocial
Problems Associated with Multiple Sclerosis:
Results from a Half-day Workshop
Intervention. Int J MS Care 2010;12(4):200-6.
30. Pakenham K, Ryan A, Mawdsley M, Brown F.
Evaluation of an ACT Resilience Training
Program (READY) for People with Diabetes
or Multiple Sclerosis. Paper presented at
ACBS Annual World Conference XIII,
Minneapolis, MN; 2014.
31. Davis ML, Morina N, Powers MB, Smits JA,
Emmelkamp PM. A Meta-analysis of the
Efficacy of Acceptance and Commitment
Therapy for Clinically Relevant Mental and
Physical Health Problems. Psychother.
Psychosom 2014;84(1):30-6.
32. Lunde L, Nordhus I. Combining Acceptance
and Commitment Therapy and Cognitive
Behavioral Therapy for the Treatment of
Chronic Pain in Older Adults. Clin Case Studi
2009;8(4):296-308.
33. Hayes SC, Levin ME, Plumb-Vilardaga J,
Villate JL, Pistorello J. Acceptance and
Commitment Therapy and Contextual
Behavioral Science: Examining the Progress of
a Distinctive Model of Behavioral and
Cognitive Therapy. Behav Ter 2013;44(2):180-
98.
34. van der Spek N, Vos J, van Uden-Kraan CF,
Breitbart W, Cuijpers P, Knipscheer-Kuipers
K, et al. Effectiveness and Cost-effectiveness
of Meaning-centered Group Psychotherapy in
Cancer Survivors: Protocol of a Randomized
Controlled Trial. BMC Psychiatry
2014;14(1):22.
35. Gagnon P, Fillion L, Robitaille MA, Girard M,
Tardif F, Cochrane JP, et al. A Cognitive–
existential Intervention to Improve Existential
and Global Quality of Life in Cancer Patients:
a Pilot Study. Palliative and Supportive Care
2015;13(04):981-90.
36. Dobríkova P, Pcolkova D, Al Turabi LK, West
Jr DJ. The Effect of Social Support and
Meaning of Life on the Quality of Life Care
for Terminally Ill patients. Am. J. Hosp.
Palliat. Med 2014,22:56- 85.
37. Breitbart W, Rosenfeld B, Gibson C, Pessin H,
Poppito S, Nelson C, et al. Meaning‐centered
Group Psychotherapy for Patients with
Advanced Cancer: a Pilot Randomized
Controlled Trial. Psycho‐Oncology.
2010;19(1):21-8.
38. Jamali F. The Relationship between Religious
Attitudes, Signifying a Sense of Life and
Mental Health in Students of Tehran
University. Psychol J Tehran AlzahraUni
2002;32:152-63. [Text in Persian]
39. Kyung Sh, Jaeim I, Heesu K, Shinjeong K,
Mikyung S, Songyong S. The Effect of
logotherapy on the Suffering, Finding
Meaning, and Spiritual Well-being of
Adolescents with Terminal Cancer. J Korean
Acad Chid Health Nurse 2009;15:136-44.
40. Pourebrahim T, Rasouli R. Effect of Group
Logotherapy on Decreasing Depression and
Increasing Meaning in Life on Older Adults
Resident in Sanitarium. J Appl Psychol
2008;2:673-85. [Text in Persian]
Discussion
The present study aimed to compare the effectiveness of acceptance and commitment group therapy and group logotherapy in reducing perceived stress among MS patients. Based on the results, both therapies were effective in reducing perceived stress among MS patients, i.e. both groups had a lower perceived stress than the control group following the interventions. Results also showed that ACT had a greater effect than logotherapy on reducing perceived stress among these patients. In line with the present study, a number of studies suggest that ACT can improve MS symptoms (28,29,30,31). ACT may have the effect by changing the patients’ attitude in the first sessions. In addition, ACT works by creating and developing “acceptance” and “enhancing value-based action” in patients (32). Contrary to other therapies, ACT imposes no specific value or lifestyle on patients. Here, patients decide to change based on their own value system. Attention to committed action is another process highlighted in this treatment protocol for MS patients. Encouraging patients to clarify values, determine goals, predict obstacles and, in the end, commit to actions for achieving those goals based on values despite the disease, saves the patients from repetitive negative thoughts and feelings, helps them realize their goals, and leads to happiness, thereby reduce stress (33). Results also revealed that group logotherapy successfully educed perceived stress in these patients. This finding is consistent with numerous studies showing the effectiveness of logotherapy in patients’ and healthy individuals’ physical and mental health (34,35,36,37). Setting goals and finding meaning of life can help MS patients overcoming symptoms such as anxiety, stress, and hopelessness (18), as hopelessness exacerbates symptoms and increases stress in them. Therefore, psychological interventions which aim to promote hope, meaning, and goals in life can be useful for this group (38). Furthermore, finding meaning reduces psychological pressures and the negative outcomes of the disease, thereby enhances mental health and adjustment. Logotherapy helps patients to stop focusing on what has been lost and, instead, search for meaning despite hopelessness. Thus, according to logotherapy, life always has meaning, and these patients can cope better under stressful situations. What matters in logotherapy is the confirmation of unique human potentials which can turn tragedies into personal victories and change unpleasant situations into pleasant ones (39). Frankl believes that,in the face of unchangeable situations such as an incurable disease, people have the opportunity to find the deepest and greatest meaning of life and thus cope with stressful and unpleasant conditions (40). These results can have important clinical implications for MS patients; the use of complementary psychological therapies together with pharmacotherapy can be more effective for patients while decreasing the costs of treatment. Moreover, the use of ACT group therapy and group logotherapy can enhance their ability to cope with unpleasant conditions and stresses caused during the course of the disease, thereby creating a better condition for them. Another result of the present study was the further effectiveness of ACT compared to logotherapy in reducing perceived stress among MS patients. The use of more behavioral and performance exercises in ACT may have resulted in its superiority. Although group logotherapy had significant effects, better results may be achieved using behavioral exercises and encouraging MS patients to utilize performance techniques.
Conclusion
The present study had certain limitations,including the lack of total control over variables such as environmental, personal, familial, psychological, and physical factors (e.g. issues related to disease relapse and medications), a number of which were, nevertheless, identified and controlled by the researchers. Moreover, limiting the population to those who were members of Iran MS Society may limit the generalizability of results to other patients. In addition, due to the adverse physical and psychological conditions of a large number of patients as well as problems which could arise as a result of their participation, the researchers had to assign a small number of subjects to each group. We recommend that future studies recruit MS patients who are not members of Iran MS Society. Also, based on the effectiveness of ACT group therapy and logotherapy in reducing perceived stress, we suggest that experts include these methods in their treatments Conflict of Interest The authors have no conflict of interest.
References
1. Halper J, Holland NJ. Multiple Sclerosis: A Self-Care Guide to Wellness. Demos Medical Publishing; 2005.
2. Mitchell AJ, Benito-León J, González JM, Rivera-Navarro J. Quality of Life and Its Assessment in Multiple Sclerosis: Integrating Physical and Psychological Components of Wellbeing. Lancet Neurol 2005;4(9):556-66.
3. Aleyasin H, Sarai A, Alaeddini F,Ansarian E, Lotfi J, Sanati MH. Multiple Sclerosis: a Study of 318 Cases. Arch Tran Med 2012; 5:249.
4. MCcabe MP. Mood and Self-esteem of Persons with Multiple Sclerosis Following an Exacerbation. J Psychosom Res 2005;59(3):161-6.
5. Ghafari S, Ahmadi F, Nabavi SM, Memarian R. Effect of Progressive Muscle Relaxation on Depression, Anxiety and Stress in Patients with MS. Res Med J Shahid Beheshti Uni Med Sci Health 2008;32: 45-53. [Text in Persian].
6. Beiske AG, Svensson E, Sandanger I, Czujko B, Pederson ED, Aarseth JH, et al. Depression and Anxiety amongst Multiple Sclerosis Patients. Eur J Neurol 2008; 15(3):239-45.
7. Yamout B, Itani S, Hourany R, Sibaii AM,Yaghi S. The Effect of War Stress on Multiple Sclerosis Exacerbations and Radiological Disease Activity. J Neurol Sci 2010;288(1- 2):42-4.
8. Mohr DC, Goodkin DE, Bacchetti P,Boudewyn AC, Huang L, Marrietta P, et al. Psychological Stress and the Subsequent Appearance of New Brain MRI Lesions in MS. Neurology2000;55(1):55-61
9. Heesen C, Mohr DC, Huitinga I, Bergh FT, Gaab J, Otte C, et al. Stress Regulation in Multiple Sclerosis Current Issues and Concepts. Mult Scler 2007;13(2):143-8.
10. Gold SM, Mohr DC, Huitinga I, Flachenecker P, Sternberg EM, Heesen C. The Role of Stress-response Systems for the Pathogenesis and Progression of MS. Trends Immunol 2005;26(12):644-52.
11. Esmonde L, Long AF. Complementary Therapy Use by Persons with Multiple Sclerosis: Benefits and Research Priorities. Complement Ther Clin Pract 2008; 14(3): 176- 84.
12. Crawford JD, McIvor GP. Group Psychotherapy: Benefits in Multiple Sclerosis. Arch Phys Med Rehabil 1985; 66: 810-3.
13. Prevedini AB, Presti G, Rabitti E, Miselli G, Moderato P. Acceptance and Commitment Therapy (ACT): the Foundation of the Therapeutic Model and an Overview of Its Contribution to the Treatment of Patients with Chronic Physical Diseases. G Ital Med Lav Ergon. 2011;33(1): A53-63.
14. Villatte JL, Vilardaga R, Villatte M, Vilardaga JC, Atkins DC, Hayes SC. Acceptance and Commitment Therapy Modules: Differential Impact on Treatment Processes and Outcomes. Behav Res Ther 2016; 77:52-61.
15. Hiratzka J, Rastegar F, Contag AG, Norvell DC, Anderson PA, Hart RA. Adverse Event Recording and Reporting in Clinical Trials Comparing Lumbar Disk Replacement with Lumbar Fusion: A Systematic Review. Global Spine J 2015;5(06):486-95.
16. Vowles KE, McCracken LM, O’Brien JZ. Acceptance and Values-based Action in Chronic Pain: a Three-year Follow-up Analysis of Treatment Effectiveness and Process. Behav Res Ter 2011;49(11):748-55.
17. Yalom ID, Leszcz M. Theory and Practice of Group Psychotherapy. Basic books; 2005.
18. Kang K, Im J, Kim H, Kim S, Song M, Sim S. The Effect of Logotherapy on the Suffering, Finding Meaning, and Spiritual Well-being of Adolescents with Terminal Cancer. Child Health Nurs Res 2009;15(2):136-44.
19. Robatmili S, Sohrabi F, Shahrak MA,Talepasand S, Nokani M, Hasani M. The Effect of Group Logotherapy on Meaning in Life and Depression Levels of Iranian Students. Int J Adv Couns 2015;37(1):54-62.
20. Bruce JM, Lynch SG. Personality Traits in Multiple Sclerosis: Association with Mood and Anxiety Disorders. J Psychosom Res 2011;70(5):479-85.
21. Burns MN, Siddique J, Fokuo JK, Mohr DC. Comorbid Anxiety Disorders and Treatment of Depression in People with Multiple Sclerosis.
22. Way SW, Popko B. Harnessing the Integrated
Stress Response for the Treatment of Multiple
Sclerosis. Lancet Neurol 2016;15(4):434-43.
23. Hayes SC, Strosahl KD, Wilson KG.
Acceptance and Commitment Therapy: An
Experiential Approach to Behavior Change.
Guilford Press; 1999.
24. Hutzell RR. A General Course of Group
Analysis. Viktor Frankl Foundation of South
Africa 2002;7:15-26.
25. Cohen S, Kamarck T. Mermelstein R. Global
Measure of Perceived Stress. Journal of Health
and Social Behavior 1983;24(4):385-96.
26. Salehi Ghadri J. Efficacy of Multiplicity of
Roles and Satisfaction with It on the Self
Esteem and Stress in Female Teachers. MA
Thesis, Tarbiat Modares University, 1994.
[Text in Persian]
27. Sepahvand T, Gilani B, Zamani R. The
Relationship between Explanatory Styles with
Perceived Stress and General Health. Journal
of Psychology and Education 2009; 38(4):27-
43. [Text in Persian]
28. Nordin L, Rorsman I. Cognitive Behavioural
Therapy in Multiple Sclerosis: a Randomized
Controlled Pilot Study of Acceptance and
Commitment Therapy. J Rehabil Med
2012;44(1):87-90.
29. Sheppard SC, Forsyth JP, Hickling EJ, Bianchi
J. A Novel Application of Acceptance and
Commitment Therapy for Psychosocial
Problems Associated with Multiple Sclerosis:
Results from a Half-day Workshop
Intervention. Int J MS Care 2010;12(4):200-6.
30. Pakenham K, Ryan A, Mawdsley M, Brown F.
Evaluation of an ACT Resilience Training
Program (READY) for People with Diabetes
or Multiple Sclerosis. Paper presented at
ACBS Annual World Conference XIII,
Minneapolis, MN; 2014.
31. Davis ML, Morina N, Powers MB, Smits JA,
Emmelkamp PM. A Meta-analysis of the
Efficacy of Acceptance and Commitment
Therapy for Clinically Relevant Mental and
Physical Health Problems. Psychother.
Psychosom 2014;84(1):30-6.
32. Lunde L, Nordhus I. Combining Acceptance
and Commitment Therapy and Cognitive
Behavioral Therapy for the Treatment of
Chronic Pain in Older Adults. Clin Case Studi
2009;8(4):296-308.
33. Hayes SC, Levin ME, Plumb-Vilardaga J,
Villate JL, Pistorello J. Acceptance and
Commitment Therapy and Contextual
Behavioral Science: Examining the Progress of
a Distinctive Model of Behavioral and
Cognitive Therapy. Behav Ter 2013;44(2):180-
98.
34. van der Spek N, Vos J, van Uden-Kraan CF,
Breitbart W, Cuijpers P, Knipscheer-Kuipers
K, et al. Effectiveness and Cost-effectiveness
of Meaning-centered Group Psychotherapy in
Cancer Survivors: Protocol of a Randomized
Controlled Trial. BMC Psychiatry
2014;14(1):22.
35. Gagnon P, Fillion L, Robitaille MA, Girard M,
Tardif F, Cochrane JP, et al. A Cognitive–
existential Intervention to Improve Existential
and Global Quality of Life in Cancer Patients:
a Pilot Study. Palliative and Supportive Care
2015;13(04):981-90.
36. Dobríkova P, Pcolkova D, Al Turabi LK, West
Jr DJ. The Effect of Social Support and
Meaning of Life on the Quality of Life Care
for Terminally Ill patients. Am. J. Hosp.
Palliat. Med 2014,22:56- 85.
37. Breitbart W, Rosenfeld B, Gibson C, Pessin H,
Poppito S, Nelson C, et al. Meaning‐centered
Group Psychotherapy for Patients with
Advanced Cancer: a Pilot Randomized
Controlled Trial. Psycho‐Oncology.
2010;19(1):21-8.
38. Jamali F. The Relationship between Religious
Attitudes, Signifying a Sense of Life and
Mental Health in Students of Tehran
University. Psychol J Tehran AlzahraUni
2002;32:152-63. [Text in Persian]
39. Kyung Sh, Jaeim I, Heesu K, Shinjeong K,
Mikyung S, Songyong S. The Effect of
logotherapy on the Suffering, Finding
Meaning, and Spiritual Well-being of
Adolescents with Terminal Cancer. J Korean
Acad Chid Health Nurse 2009;15:136-44.
40. Pourebrahim T, Rasouli R. Effect of Group
Logotherapy on Decreasing Depression and
Increasing Meaning in Life on Older Adults
Resident in Sanitarium. J Appl Psychol
2008;2:673-85. [Text in Persian]
Type of Study: Research |
Subject:
Special
Received: 2017/10/16 | Accepted: 2017/10/16 | Published: 2017/10/16
Received: 2017/10/16 | Accepted: 2017/10/16 | Published: 2017/10/16
References
1. Halper J, Holland NJ. Multiple Sclerosis: A Self-Care Guide to Wellness. Demos Medical Publishing; 2005.
2. Mitchell AJ, Benito-León J, González JM, Rivera-Navarro J. Quality of Life and Its Assessment in Multiple Sclerosis: Integrating Physical and Psychological Components of Wellbeing. Lancet Neurol 2005;4(9):556-66. [DOI:10.1016/S1474-4422(05)70166-6]
3. Aleyasin H, Sarai A, Alaeddini F,Ansarian E, Lotfi J, Sanati MH. Multiple Sclerosis: a Study of 318 Cases. Arch Tran Med 2012; 5:249.
4. MCcabe MP. Mood and Self-esteem of Persons with Multiple Sclerosis Following an Exacerbation. J Psychosom Res 2005;59(3):161-6. [DOI:10.1016/j.jpsychores.2005.04.010] [PMID]
5. Ghafari S, Ahmadi F, Nabavi SM, Memarian R. Effect of Progressive Muscle Relaxation on Depression, Anxiety and Stress in Patients with MS. Res Med J Shahid Beheshti Uni Med Sci Health 2008;32: 45-53. [Text in Persian].
6. Beiske AG, Svensson E, Sandanger I, Czujko B, Pederson ED, Aarseth JH, et al. Depression and Anxiety amongst Multiple Sclerosis Patients. Eur J Neurol 2008; 15(3):239-45. [DOI:10.1111/j.1468-1331.2007.02041.x] [PMID]
7. Yamout B, Itani S, Hourany R, Sibaii AM, Yaghi S. The Effect of War Stress on Multiple Sclerosis Exacerbations and Radiological Disease Activity. J Neurol Sci 2010;288(1-2):42-4. [DOI:10.1016/j.jns.2009.10.012] [PMID]
8. Mohr DC, Goodkin DE, Bacchetti P, Boudewyn AC, Huang L, Marrietta P, et al. Psychological Stress and the Subsequent Appearance of New Brain MRI Lesions in MS. Neurology2000;55(1):55-61 [DOI:10.1212/WNL.55.1.55] [PMID]
9. Heesen C, Mohr DC, Huitinga I, Bergh FT, Gaab J, Otte C, et al. Stress Regulation in Multiple Sclerosis Current Issues and Concepts. Mult Scler 2007;13(2):143-8. [DOI:10.1177/1352458506070772] [PMID]
10. Gold SM, Mohr DC, Huitinga I, Flachenecker P, Sternberg EM, Heesen C. The Role of Stress-response Systems for the Pathogenesis and Progression of MS. Trends Immunol 2005;26(12):644-52. [DOI:10.1016/j.it.2005.09.010] [PMID]
11. Esmonde L, Long AF. Complementary Therapy Use by Persons with Multiple Sclerosis: Benefits and Research Priorities. Complement Ther Clin Pract 2008; 14(3): 176-84. [DOI:10.1016/j.ctcp.2008.03.001] [PMID]
12. Crawford JD, McIvor GP. Group Psychotherapy: Benefits in Multiple Sclerosis. Arch Phys Med Rehabil 1985; 66: 810-3. [PMID]
13. Prevedini AB, Presti G, Rabitti E, Miselli G, Moderato P. Acceptance and Commitment Therapy (ACT): the Foundation of the Therapeutic Model and an Overview of Its Contribution to the Treatment of Patients with Chronic Physical Diseases. G Ital Med Lav Ergon. 2011;33(1): A53-63. [PMID]
14. Villatte JL, Vilardaga R, Villatte M, Vilardaga JC, Atkins DC, Hayes SC. Acceptance and Commitment Therapy Modules: Differential Impact on Treatment Processes and Outcomes. Behav Res Ther 2016; 77:52-61. [DOI:10.1016/j.brat.2015.12.001] [PMID] [PMCID]
15. Hiratzka J, Rastegar F, Contag AG, Norvell DC, Anderson PA, Hart RA. Adverse Event Recording and Reporting in Clinical Trials Comparing Lumbar Disk Replacement with Lumbar Fusion: A Systematic Review. Global Spine J 2015;5(06):486-95. [DOI:10.1055/s-0035-1567835] [PMID] [PMCID]
16. Vowles KE, McCracken LM, O'Brien JZ. Acceptance and Values-based Action in Chronic Pain: a Three-year Follow-up Analysis of Treatment Effectiveness and Process. Behav Res Ter 2011;49(11):748-55. [DOI:10.1016/j.brat.2011.08.002] [PMID]
17. Yalom ID, Leszcz M. Theory and Practice of Group Psychotherapy. Basic books; 2005.
18. Kang K, Im J, Kim H, Kim S, Song M, Sim S. The Effect of Logotherapy on the Suffering, Finding Meaning, and Spiritual Well-being of Adolescents with Terminal Cancer. Child Health Nurs Res 2009;15(2):136-44. [DOI:10.4094/jkachn.2009.15.2.136]
19. Robatmili S, Sohrabi F, Shahrak MA, Talepasand S, Nokani M, Hasani M. The Effect of Group Logotherapy on Meaning in Life and Depression Levels of Iranian Students. Int J Adv Couns 2015;37(1):54-62. [DOI:10.1007/s10447-014-9225-0] [PMID] [PMCID]
20. Bruce JM, Lynch SG. Personality Traits in Multiple Sclerosis: Association with Mood and Anxiety Disorders. J Psychosom Res 2011;70(5):479-85. [DOI:10.1016/j.jpsychores.2010.12.010] [PMID]
21. Burns MN, Siddique J, Fokuo JK, Mohr DC. Comorbid Anxiety Disorders and Treatment of Depression in People with Multiple Sclerosis. Rehabil Psychol 2010;55(3):255-62. [DOI:10.1037/a0020492] [PMID] [PMCID]
22. Way SW, Popko B. Harnessing the Integrated Stress Response for the Treatment of Multiple Sclerosis. Lancet Neurol 2016;15(4):434-43. [DOI:10.1016/S1474-4422(15)00381-6]
23. Hayes SC, Strosahl KD, Wilson KG. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change. Guilford Press; 1999.
24. Hutzell RR. A General Course of Group Analysis. Viktor Frankl Foundation of South Africa 2002;7:15-26.
25. Cohen S, Kamarck T. Mermelstein R. Global Measure of Perceived Stress. Journal of Health and Social Behavior 1983;24(4):385-96. [DOI:10.2307/2136404] [PMID]
26. Salehi Ghadri J. Efficacy of Multiplicity of Roles and Satisfaction with It on the Self Esteem and Stress in Female Teachers. MA Thesis, Tarbiat Modares University, 1994. [Text in Persian]
27. Sepahvand T, Gilani B, Zamani R. The Relationship between Explanatory Styles with Perceived Stress and General Health. Journal of Psychology and Education 2009; 38(4):27-43. [Text in Persian]
28. Nordin L, Rorsman I. Cognitive Behavioural Therapy in Multiple Sclerosis: a Randomized Controlled Pilot Study of Acceptance and Commitment Therapy. J Rehabil Med 2012;44(1):87-90. [DOI:10.2340/16501977-0898] [PMID]
29. Sheppard SC, Forsyth JP, Hickling EJ, Bianchi J. A Novel Application of Acceptance and Commitment Therapy for Psychosocial Problems Associated with Multiple Sclerosis: Results from a Half-day Workshop Intervention. Int J MS Care 2010;12(4):200-6. [DOI:10.7224/1537-2073-12.4.200]
30. Pakenham K, Ryan A, Mawdsley M, Brown F. Evaluation of an ACT Resilience Training Program (READY) for People with Diabetes or Multiple Sclerosis. Paper presented at ACBS Annual World Conference XIII, Minneapolis, MN; 2014.
31. Davis ML, Morina N, Powers MB, Smits JA, Emmelkamp PM. A Meta-analysis of the Efficacy of Acceptance and Commitment Therapy for Clinically Relevant Mental and Physical Health Problems. Psychother. Psychosom 2014;84(1):30-6. [PMID]
32. Lunde L, Nordhus I. Combining Acceptance and Commitment Therapy and Cognitive Behavioral Therapy for the Treatment of Chronic Pain in Older Adults. Clin Case Studi 2009;8(4):296-308. [DOI:10.1177/1534650109337527]
33. Hayes SC, Levin ME, Plumb-Vilardaga J, Villate JL, Pistorello J. Acceptance and Commitment Therapy and Contextual Behavioral Science: Examining the Progress of a Distinctive Model of Behavioral and Cognitive Therapy. Behav Ter 2013;44(2):180-98. [DOI:10.1016/j.beth.2009.08.002] [PMID] [PMCID]
34. van der Spek N, Vos J, van Uden-Kraan CF, Breitbart W, Cuijpers P, Knipscheer-Kuipers K, et al. Effectiveness and Cost-effectiveness of Meaning-centered Group Psychotherapy in Cancer Survivors: Protocol of a Randomized Controlled Trial. BMC Psychiatry 2014;14(1):22. [DOI:10.1186/1471-244X-14-22] [PMID] [PMCID]
35. Gagnon P, Fillion L, Robitaille MA, Girard M, Tardif F, Cochrane JP, et al. A Cognitive–existential Intervention to Improve Existential and Global Quality of Life in Cancer Patients: a Pilot Study. Palliative and Supportive Care 2015;13(04):981-90. [DOI:10.1017/S147895151400073X] [PMID] [PMCID]
36. Dobríkova P, Pcolkova D, Al Turabi LK, West Jr DJ. The Effect of Social Support and Meaning of Life on the Quality of Life Care for Terminally Ill patients. Am. J. Hosp. Palliat. Med 2014,22:56- 85.
37. Breitbart W, Rosenfeld B, Gibson C, Pessin H, Poppito S, Nelson C, et al. Meaning‐centered Group Psychotherapy for Patients with Advanced Cancer: a Pilot Randomized Controlled Trial. Psycho‐Oncology. 2010;19(1):21-8. [DOI:10.1002/pon.1556] [PMID] [PMCID]
38. Jamali F. The Relationship between Religious Attitudes, Signifying a Sense of Life and Mental Health in Students of Tehran University. Psychol J Tehran AlzahraUni 2002;32:152-63. [Text in Persian]
39. Kyung Sh, Jaeim I, Heesu K, Shinjeong K, Mikyung S, Songyong S. The Effect of logotherapy on the Suffering, Finding Meaning, and Spiritual Well-being of Adolescents with Terminal Cancer. J Korean Acad Chid Health Nurse 2009;15:136-44. [DOI:10.4094/jkachn.2009.15.2.136]
40. Pourebrahim T, Rasouli R. Effect of Group Logotherapy on Decreasing Depression and Increasing Meaning in Life on Older Adults Resident in Sanitarium. J Appl Psychol 2008;2:673-85. [Text in Persian]
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
