Tue, Apr 23, 2024
Volume 8, Issue 2 (Spring 2022)
Caspian J Neurol Sci 2022, 8(2): 104-116 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dastoorpoor M, Khodadadi N, Majdinasab N, Soltani M, Ghanbari S. The Time-trend of Multiple Sclerosis Incidence and Prevalence in Khuzestan Province, Iran. Caspian J Neurol Sci 2022; 8 (2) :104-116
URL: http://cjns.gums.ac.ir/article-1-520-en.html
URL: http://cjns.gums.ac.ir/article-1-520-en.html



1- Department of Biostatistics and Epidemiology, Musculoskeletal Rehabilitation Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
2- Department of Neurology, Musculoskeletal Rehabilitation Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
3- Department of Speech Therapy, School of Rehabilitation Sciences, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
4- Department of Biostatistics and Epidemiology, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
2- Department of Neurology, Musculoskeletal Rehabilitation Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
3- Department of Speech Therapy, School of Rehabilitation Sciences, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
4- Department of Biostatistics and Epidemiology, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Full-Text [PDF 2279 kb]
(386 Downloads)
| Abstract (HTML) (892 Views)
Full-Text: (385 Views)
Introduction
Multiple Sclerosis (MS) frequency distribution is measured by estimating prevalence and incidence. To determine the relative contribution of genetic and environmental factors in the development of MS, related studies compared the prevalence and incidence of MS among different populations [1]. The incidence rate of the disease refers to the number of new cases over some time (usually one year), while the prevalence rate refers to the number of individuals with the disease (usually per 100000 individuals). According to the latest update of Assessment of the MS Outbreak by the Atlas of MS, i.e., the most widely used source worldwide for MS epidemiology with universal access to resources for individuals with MS; the estimated number of individuals with MS in 2008 was 2.1 million subjects which increased to 2.3 million people in 2013. Moreover, the global average prevalence increased from 30 in 2008 to 33 per 100000 individuals in 2013 [2].
Recently, Iran has become a country with a high prevalence, and the prevalence continues to increase [3, 4, 5]. The study conducted by Hosseinzadeh et al. found that Iran is a high-risk area as regards MS. The MS incidence and the ratio of women to men (average annual incidence: 6.7 per 100000 individuals; the ratio of women to men: 10.5 & 3.0) are comparable to the dominant patterns in the developed countries [6]. In another study published at the end of July 2020, Abtahi et al. found that the frequency distribution of MS prevalence ranged from 7.40 to 101.39 per 100000 individuals. Twenty-One provinces in Iran are at high risk of MS (>25 per 100000 individuals), and 9 provinces are at moderate risk (5-25 per 100000 individuals) [7]. Despite several cross-sectional studies describing the past trend of the disease in Iran, studies related to predicting its prevalence and incidence in the coming years are few. A survey in Kohgiluyeh and Boyer-Ahmad Province used the curve estimation method to examine changes in the prevalence and incidence of the disease, and the univariate time series model for analysis [8]. Another study in Canada used a population-based longitudinal, micro-simulation model named POHEM-Neurological for identifying individuals with MS and for future prognosis and MS mortality. They used the incidence and mortality parameters of a British Columbia-based group [9].
The prevalence of MS is on the rise. Accordingly, addressing the issue of prevalence and incidence and focusing on the models of predicting the trend of MS could be helpful. Such data can be valuable in planning for the current situation, getting ready for unexpected conditions in the coming years, assessing the speed of disease spread, and identifying strategies for its prevention and treatment [8]. Therefore, this study performed an epidemiological analysis on the temporal trends of the prevalence and incidence rate of MS (2006-2019). Furthermore, we proposed a prognosis model for MS prevalence and incidence in Khuzestan Province based on data collected from the Khuzestan Multiple Sclerosis Center.
Materials and Methods
Khuzestan Province is located at the coast of the Persian Gulf in the southwest of Iran. It is considered the center of Iran’s oil and gas production. The area of this province is 64.055 square kilometers with a population of more than 4.711 million (according to the 2016 census), is the fifth most populous province in Iran [10]. Khuzestan Province is located at 31.33˚N and 48.69 ˚E (Figure 1)..jpg) All study data were extracted from the database of the Khuzestan MS Center. Khuzestan MS Center records information concerning MS patients from all parts of the province after the final diagnosis. The Khuzestan MS Center is in Ahvaz Jundishapur University of Medical Sciences. It is a referral for all patients residing in Khuzestan Province whose disease is diagnosed for the first time by neurologists. In the center, MS patients are evaluated by neurologists supervising the MS Center, and the final diagnosis is confirmed based on clinical and radiological evidence. Patient data in this study included the following: age, diagnosis age, duration, the first symptom of the disease, sex, education, employment status, race, marital status, and MS type. These data were retrieved from the database of the Khuzestan Multiple Sclerosis Center since the establishment of this association since 2006 entered the study by the end of 2019. To estimate the prevalence and incidence of MS by gender (female, male) and age groups (under 20, 20-50 years, & over 50 years) in different years according to the census, the study used census population. However, to obtain the number of populations between the census years, the natural population growth rate in the base population was used. The simple exponential smoothing model was used to study time-trends and predict the prevalence and incidence of MS, in Khuzestan, in 2020.
All study data were extracted from the database of the Khuzestan MS Center. Khuzestan MS Center records information concerning MS patients from all parts of the province after the final diagnosis. The Khuzestan MS Center is in Ahvaz Jundishapur University of Medical Sciences. It is a referral for all patients residing in Khuzestan Province whose disease is diagnosed for the first time by neurologists. In the center, MS patients are evaluated by neurologists supervising the MS Center, and the final diagnosis is confirmed based on clinical and radiological evidence. Patient data in this study included the following: age, diagnosis age, duration, the first symptom of the disease, sex, education, employment status, race, marital status, and MS type. These data were retrieved from the database of the Khuzestan Multiple Sclerosis Center since the establishment of this association since 2006 entered the study by the end of 2019. To estimate the prevalence and incidence of MS by gender (female, male) and age groups (under 20, 20-50 years, & over 50 years) in different years according to the census, the study used census population. However, to obtain the number of populations between the census years, the natural population growth rate in the base population was used. The simple exponential smoothing model was used to study time-trends and predict the prevalence and incidence of MS, in Khuzestan, in 2020.
The simplest exponential smoothing method is called Simple Exponential Smoothing (SES) (in some books, it is called “single exponential smoothing”). It can be viewed either as an adaptive-forecasting algorithm. Exponential smoothing is implemented to predict a time series with no linear trend and seasonal pattern. The observation of the short-range time series has an aperiodic variation and fluctuates around a stable mean over time. The equation for this method is as follows:
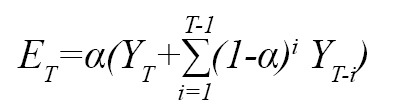
The YT and ET are the observed and forecasted value of the series at time T, and α is the smoothing constant. The above equation shows that the method constructs a weighted average of the observations [11, 12, 13], introducing single-exponential smoothing as a modern time-series method. It can produce optimal forecasts for several underlying models, including ARIMA (0,1,1) and the random-walk-plus-noise and state-space models [13].
The procedures of the Single Exponential Smoothing Method (SESM) are presented as per below:
Step 1: Compute the initial estimate of the series at period t=0.
There is no theoretical justification for estimating the initial values. It is common to calculate initial estimates of exponential smoothing procedures using historical data; however, it is not applicable in all situations. Setting it to Y1 is a method of initialization. The average of the first four or 5 observations could be another possible way of initialization.
Step 2: Compute the updated estimate using the smoothing equation.

The smoothing parameter or smoothing constant that takes values between zero and one. Note that:
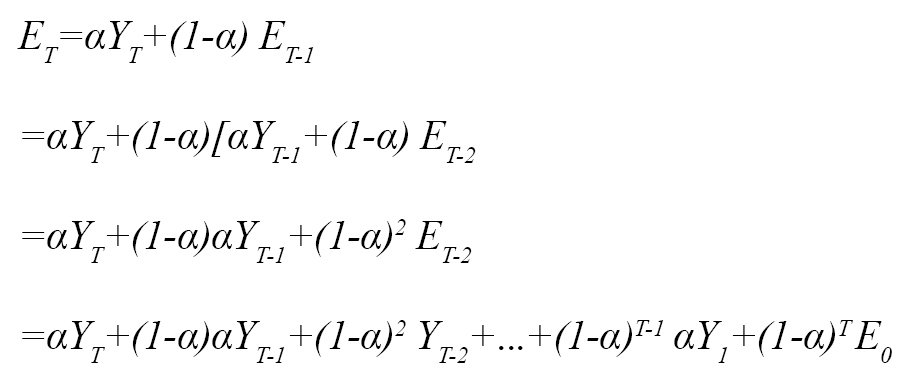
The coefficients measuring the contributions of the observations decrease exponentially over time. The smoothing parameter controls the trade-off between the closeness of smoothed data to the observed data.
Although there is no generally accepted statistical procedure for choosing α, a small value for α., i.e., close to 0, has a greater smoothing effect and weighs the more distant past observations. In contrast, the value of close to one gives more weight to the recent observations. As a great suggestion to choose α, the value that made smaller Root Mean Square Error (RMSE) of the forecast, the square root of squared deviations between the forecasts and the
realized values could be a proper selection. Eventually, we used the Augmented Dickey-Fuller test for unit root to find the stationary of the data. All analysis was done by Stata12 software.
The simple exponential smoother is a special case of a simple moving average. In the moving average, all data points are assigned equal weights. Arguably, recent observation provides more relevant information than the observation in the past. Therefore, the exponential-smoothing method can give larger weights to more recent observations, and weight decreases exponentially as the observation becomes more distant. This method is more effective when the observations change slowly over time. The simple exponential smoothing method is used for short-range forecasting, usually just one lag into the future.
Results
In total, 2676 patients with MS were registered in the Khuzestan Multiple Sclerosis Center from its establishment (2006) until the end of December 2019, i.e., included in the study. The mean and SD score for the MS patients’ age was 31.40 and 8.94 years. The youngest and oldest patients were 10 and 75 years old, respectively. The sex ratio (female to male) was 3.05, meaning that one-third of the patients were male. The mean±SD age of incidence of MS was 29.19±9.16 years. Overall, 75% of patients were under 35 years of age at diagnosis. The majority had post-diploma and bachelor’s degrees (35.10%), were married (62.10%), and concerning ethnicity, were Lor (34.50%). In terms of the type of MS, RRMS was the most common type among the patients (76.3%); however, only 3.5% had the PPMS type, and 4.9% had the SPMS type (Table 1). Other details are presented in Table 1.
.jpg)
Table 2 shows the number of patients with MS and the total population by gender in different years of the study.
.jpg)
Overall, the prevalence and average annual incidence of MS disease were 57.77 and 4.35 per 100000 individuals from 2006 to 2019, respectively.
The estimated incidence and prevalence rate per 100000 individuals are displayed in Table 3.
.jpg)
We used the single exponential smoothing method to consider these time series data and forecast appropriately. In this regard, to have a minimum Root Mean Square Error (RMSE) for incidence and prevalence rate, the smoothing constant α is equal to 0.75 and 0.9, respectively. The first observation was used as the initial value. The trend of incidence and prevalence rate in total population, females, and males are shown in Table 3 and Figures 2 and 3. The forecasting of incidence and prevalence rate in 2020 is reported in Table 3. The study used the Augmented Dickey-Fuller test for unit root to check the linear trend and find the data’s stationery. The data for incidence had stationary in all categories. For prevalence data, the unit root test shows no stationary, i.e., attributed to the increasing nature of this data type.
The trend of incidence rate changes in Figure 2 represents that the incidence rate in females is higher than males in all years.
.jpg)
However, these rates get closer at the beginning of 2006, in the middle at the end of 2013, and 2019. We predict that the incidence rate in 2020 will be more or less similar to 2019 in total and for both generations.
The trend of incidence rate changes in Figure 2 represents that the incidence rate in females is higher than males in all years. However, these rates get closer at the beginning in 2006, in the middle in 2013, and at the end in 2019.
The prevalence rate changes in Figure 3 represent that multiple sclerosis is more prevalent in males.
.jpg)
The graph shows that the prevalence rate gets more over time. However, the increasing slope is higher for women. Our forecast for the prevalence is the same for 2020 compared to 2019.
MS, from 2006 to 2019, is more prevalent in individuals aged between twenty to fifty years old in Khuzestan province. The new cases and total populations in a 3-age category are displayed in Table 4.
.jpg)
The estimated incidence and prevalence rate per 100000 individuals for the three-age categories are in Table 3. The single exponential smoothing method was used to consider these time series data. To minimize the MSE and properly forecast the incidence and prevalence rate, the smoothing constant α is equal to 0.7 and 0.95, respectively. The estimated smoothing values can be seen in Table 5 and Figures 4 and 5. The forecasting of incidence and prevalence rate in 2020 is reported in Table 5.
.jpg)
To check the linear trend and find the data’s stationery, we used the Augmented Dickey-Fuller test for unit root. It showed that the data for incidence had stationary in all categories. For prevalence data, the test of the unit root shows no stationery.
The incidence rate of MS in three age categories is represented in Figure 4.
.jpg)
As we consider for individuals under 20 and above 50 years old, the incidence rate of MS had increased just slightly over time and is less than 2 per 100000 individuals. In the 20 to 50 years old individuals, the incidence rate is higher and close to 8 per 100000 individuals. We forecast that the incidence rate will increase slightly in 2020 than 2019, just for the 20-50 age category.
Figure 5 represents that MS’s prevalence rate is very high for between twenty to fifty people.
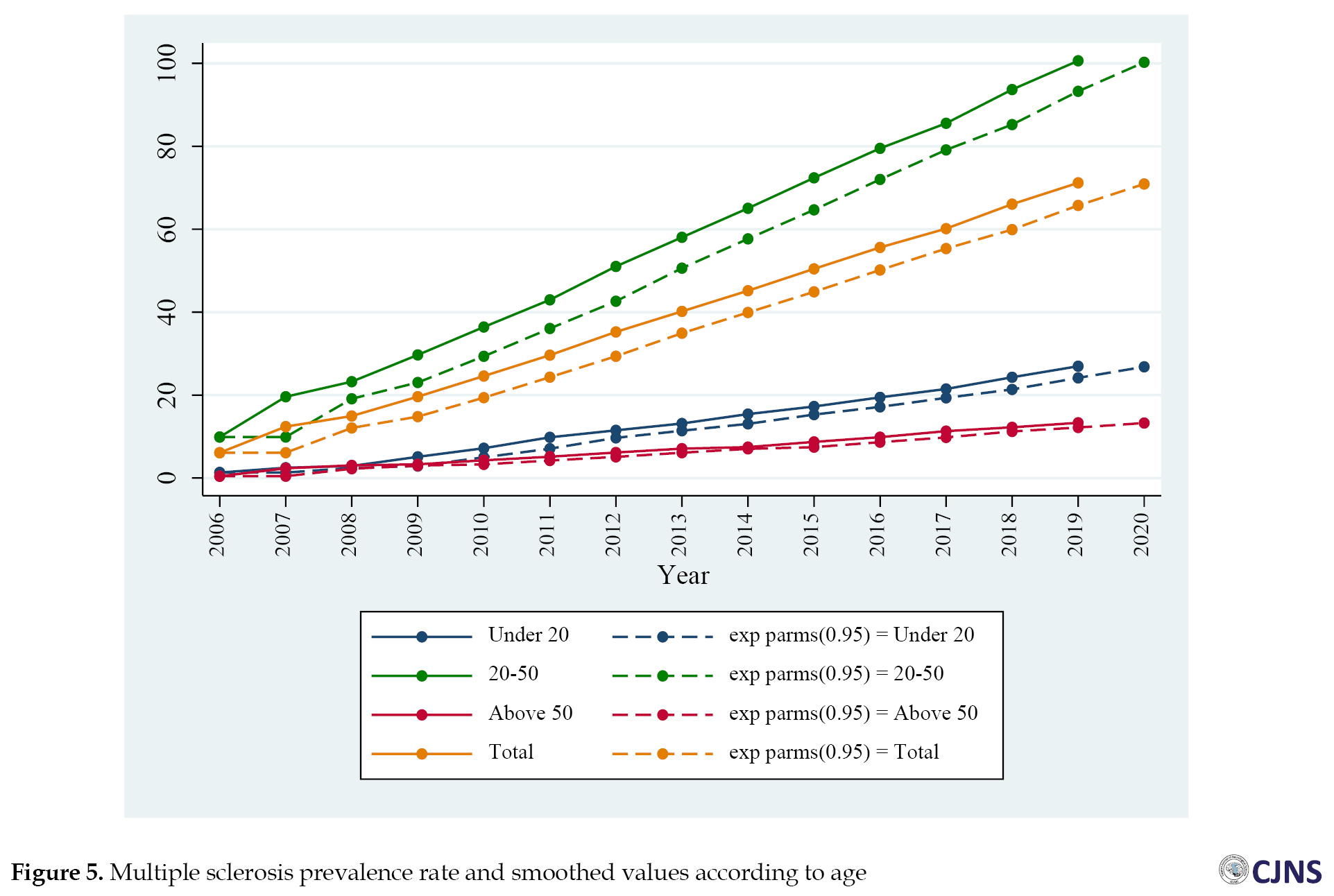
It gets more over time; however, the increasing slope is much higher for individuals aged 20 to 50. The increase in the prevalence rate of MS for under 20 years of age and above 50 has a slight slope. Moreover, our forecast for the prevalence is the same for 2020 compared to 2019 in 3 age categories.
Discussion
Our results indicated that the patients’ prevalence and average annual incidence were 57.77 and 4.35 per 100000 people from 2006 to 2019, respectively. Therefore, Khuzestan has been one of the high-risk areas for MS (prevalence of >25 per 100000 subjects).
MS prevalence and incidence have been increasing over time. Meanwhile, there is a slight change in the annual incidence of MS from 5.01 per 100000 individuals in 2006 to 4.87 per 100000 subjects in 2019. The slope of the increase in all years (from 2006 to 2019) has been higher for women than men. The number of new cases and the total population of women with MS is almost three times higher than men. However, this ratio was closer in the early years (2006), in 2013, and later in 2019. The MS incidence in women and men had increased slightly from 7.14 and 2.78 per 100000 individuals in 2006 to 7.17and 2.49 per 100000 individuals in 2019, respectively.
In 2008, we observed a decrease in the incidence. One of the significant reasons for this decrease in 2008 was the occurrence of dust in Khuzestan province and consequently the migration of some patients to neighboring provinces, such as Isfahan and Shiraz. We later saw the names of these migrating patients in the MS registration canters of those cities.
Similarly, the prevalence of MS increased from 5.01 per 100000 individuals in 2006 to 57.77 per 100000 people in 2019. Meanwhile, the MS prevalence in females and males has increased from 7.14 and 2.78 per 100000 subjects in 2006 to 85.50 and 29.06 per 100000 subjects in 2019, respectively.
Prior to this study, two other studies investigated the prevalence or incidence of the disease in Khuzestan Province; however, in smaller populations and smaller areas. Radmehr et al. estimated the prevalence of MS in northern Khuzestan at 15 per 100000, with a female-to-male ratio of 2.08 to 1 [14]. In Sharafaddinzadeh’s study, which identified 696 patients with MS in Ahvaz (Khuzestan’s capital), the prevalence and incidence of MS were 16.28 and 2.20 per 100000, respectively [15]. In other regions of Iran, in Asmarian’s study conducted on 5468 patients with MS in Fars Province, the incidence significantly increased from 1991 and 2016. At the beginning of the study (1991), the incidence rate was 0.61, and at the end (2016), it was 11.20 per 100000 individuals, and this ratio was higher in women than men in all years studied [16]. A study aimed at estimating the prevalence and incidence of MS in the Persian Gulf region, which reviewed 39 articles published from January 1985 to December 2018 in this region, reported the average age of patients with MS as 23.11 years. The disease incidence was estimated at 5.03 per 100000 and the prevalence at 39.31 per 100000, increasing by 2.3% from 1985 to 2018 [17]. In other parts of the world, the results of a study by Patti et al. in Biancavilla, Sicily, southern Italy, suggested an increase in the average annual incidence for the period 2012-2018 (16.8 per 100000 individuals), compared to the period 1992-1996 (4.5 in 100000 subjects). As of December 31, 2018, the prevalence of the disease was 292.3 per 100000 individuals (198.2 for men & 380.7 per 100000 for women), indicating a high-risk area for MS [18]. In Brola et al.’s study in Swietokrzyskie Province (central Poland), the results were similar. The prevalence of MS on December 31, 2015, was 121.3 per 100,000 people (167.1 per 100000 women, 73.2 per 100,000 men) and the average annual incidence of MS between 2010 and 2015 was about 4.5 per 100000 individuals. This rate was estimated to be much higher than in 2010 and previous studies in Poland [19].
Concerning the MS incidence in the three age groups in the present study, for individuals under 20 and over 50 years, the incidence over time has been constant and less than 2 per 100000 subjects. While in the age group of 20 to 50 years, the incidence rate was higher and close to 8 per 100000 individuals. Our age-wise results indicated a mean age of 31.40 years for patients with MS. Moreover, 75% of patients were below 35 years of age at diagnosis.
In other studies, the prevalence and incidence at a young age have been reported more than in other age groups. In Hosseinzadeh study in Iran, the mean age of patients with MS for men and women was 31.3 and 32.3 years, respectively [6]. In Cheraghmakani’s study in Mazandaran, Iran, the highest MS incidence rate is reported among the 30-34-year-old age group (28.5 per 100000 subjects), while the lowest rate was reported for above 65-year olds (0.2 per 100000 individuals) [20]. However, in Rotstein’s study, the MS prevalence increased mainly for individuals aged 35 years and older, especially individuals over 50 years [21].
Regarding some demographic and clinical variables, including the higher MS prevalence in women and the youth and the higher prevalence of relapsing-remitting MS, the results of this study are consistent with other studies.
Another variable focused in this study was the racial-ethnic aspect of patients with MS. In this study, most individuals with MS were Lors (34.5%), Persians (33.3%), and Arabs (26.3%). In this regard, Sharafaddinzadeh’s study on the impact of Persian and Arab ethnics living in Khuzestan Province on MS it was shown that the prevalence and incidence of MS were higher in the Persian population. However, the progressive nature of MS with motor symptoms and cerebellar involvement was more common in the Arab population [15]. In our study, ocular and sensory disturbances were reported as the first MS symptom more than other symptoms. Some other studies have emphasized this [15, 22]. The relationship between occupation and MS prevalence rate survey reported the highest frequency for homemakers. This is because housewives are more than working women in Iran. The MS prevalence in people with “diplomas” and “post-diploma and bachelor” has been higher than others, indicating the dominant population of Iranian society with this level of education.
Most studies evaluated the prevalence and incidence and description of the temporal trends of MS, and few have predicted the prevalence and incidence of MS in the coming years. The present study predicted that the incidence of MS in 2020 will be more or less the same compared to 2019 and will reach 4.86 per 100000 individuals, i.e., more for women than men (7.17 & 2.47 per 100000 individuals, respectively), and only in the 20-50-year-old age group. However, it is predicted that the prevalence of MS in 2020 for all age and sex groups will be more or less the same as in 2019. In this regard, in Canada, Nana et al. reviewed and presented a prognosis model over 20 years and estimated that MS cases will increase from 4051 in 2011 to 4794 in 2031. The prevalence of MS will exceed 400 per 100000 and is 3 times more common in women than in men [9]. Likewise, in Mousavizadeh’s study in Kohgiluyeh and Boyer-Ahmad, Iran, on 421 patients between 1990 and 2016, the MS prevalence was estimated to be 60.14 per 100000 the average annual incidence was 3.8 per 100000 individuals. The MS incidence was projected to increase from 8.5 per 100000 at the end of 2016 to more than 17 per 100000 individuals in 2025, and in 2025 MS will exceed 1,250, representing a nearly threefold increase in the diagnosed cases over 10 years [8].
Several factors may increase the prevalence and incidence of MS in the region between 2006 and 2019. Despite its sunny weather, vitamin D deficiency remains among the most critical health issues in Khuzestan Province [23, 24]. Further epidemiological studies have shown that serum vitamin D deficiency can be a potential environmental predisposing factor for MS in Iran [25]. Furthermore, this area’s inhabitants encounter dust particles and high temperatures. The adverse effect of Particulate Matter of 10 (PM10) on dusty days on people’s health in Ahvaz is more than days without dust [26]. A positive association between exposure to air pollution and multiple sclerosis has been reported in some studies [27, 28, 29, 30]. Lifestyle changes, increasing urbanization, and industrialization of cities can be other factors [31]. According to studies, provinces with less urbanization, such as Sistan-Baluchestan and South Khorasan in Iran, have the lowest prevalence of MS. In contrast, provinces with high urbanization, such as Tehran and Isfahan, have the highest prevalence [32].
This study has its strengths and limitations. The first study presented the prevalence and incidence of MS and presented a predictive model in all of Khuzestan Province. On the other hand, the actual number of individuals with MS may not be identified for various reasons, as follows: The elderly with long-term illness, primarily secondary progressive MS, are few. There are problems in accessing people who rarely communicate with medical services or have difficulty communicating with a physician. In addition, some young patients with mild forms of MS might avoid contacting medical services or do not require medical treatment during the study years.
Conclusion
Khuzestan Province is a high-risk area for MS. In the province, the overall prevalence has increased from 2006 to 2019. The overall incidence has been increasing with a very slight slope. The increase in prevalence and incidence was more noticeable in women than in men. The present study also predicts an increase in the incidence of MS in the coming years in the age group of 20 to 50 years. However, MS prevalence is similar to 2019. Establishing a national registry for comprehensive long-term follow-up studies is recommended.
Ethical Considerations
Compliance with ethical guidelines
The proposal of this study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (Code: IR.AJUMS.REC.1397.640).
Funding
This study was funded and supported by Ahvaz Jundishapur University of Medical Sciences (Grant No: PHT-9727).
Authors contributions
Conceptualization, methodology, supervision and project administration: Maryam Dastoorpoor; Investigation: Nastaran Majdinasab and Majid Soltani; Writing – original draft: Narges Khodadadi; Writing – review & editing: Narges Khodadadi and Maryam Dastoorpoor; Formal analysis and software: Saeed Ghanbari and Maryam Dastoorpoor.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors wish to express their gratitude to Ms. Maryam Nedamat for her kind assistance.
Refrences
Multiple Sclerosis (MS) frequency distribution is measured by estimating prevalence and incidence. To determine the relative contribution of genetic and environmental factors in the development of MS, related studies compared the prevalence and incidence of MS among different populations [1]. The incidence rate of the disease refers to the number of new cases over some time (usually one year), while the prevalence rate refers to the number of individuals with the disease (usually per 100000 individuals). According to the latest update of Assessment of the MS Outbreak by the Atlas of MS, i.e., the most widely used source worldwide for MS epidemiology with universal access to resources for individuals with MS; the estimated number of individuals with MS in 2008 was 2.1 million subjects which increased to 2.3 million people in 2013. Moreover, the global average prevalence increased from 30 in 2008 to 33 per 100000 individuals in 2013 [2].
Recently, Iran has become a country with a high prevalence, and the prevalence continues to increase [3, 4, 5]. The study conducted by Hosseinzadeh et al. found that Iran is a high-risk area as regards MS. The MS incidence and the ratio of women to men (average annual incidence: 6.7 per 100000 individuals; the ratio of women to men: 10.5 & 3.0) are comparable to the dominant patterns in the developed countries [6]. In another study published at the end of July 2020, Abtahi et al. found that the frequency distribution of MS prevalence ranged from 7.40 to 101.39 per 100000 individuals. Twenty-One provinces in Iran are at high risk of MS (>25 per 100000 individuals), and 9 provinces are at moderate risk (5-25 per 100000 individuals) [7]. Despite several cross-sectional studies describing the past trend of the disease in Iran, studies related to predicting its prevalence and incidence in the coming years are few. A survey in Kohgiluyeh and Boyer-Ahmad Province used the curve estimation method to examine changes in the prevalence and incidence of the disease, and the univariate time series model for analysis [8]. Another study in Canada used a population-based longitudinal, micro-simulation model named POHEM-Neurological for identifying individuals with MS and for future prognosis and MS mortality. They used the incidence and mortality parameters of a British Columbia-based group [9].
The prevalence of MS is on the rise. Accordingly, addressing the issue of prevalence and incidence and focusing on the models of predicting the trend of MS could be helpful. Such data can be valuable in planning for the current situation, getting ready for unexpected conditions in the coming years, assessing the speed of disease spread, and identifying strategies for its prevention and treatment [8]. Therefore, this study performed an epidemiological analysis on the temporal trends of the prevalence and incidence rate of MS (2006-2019). Furthermore, we proposed a prognosis model for MS prevalence and incidence in Khuzestan Province based on data collected from the Khuzestan Multiple Sclerosis Center.
Materials and Methods
Khuzestan Province is located at the coast of the Persian Gulf in the southwest of Iran. It is considered the center of Iran’s oil and gas production. The area of this province is 64.055 square kilometers with a population of more than 4.711 million (according to the 2016 census), is the fifth most populous province in Iran [10]. Khuzestan Province is located at 31.33˚N and 48.69 ˚E (Figure 1).
The simplest exponential smoothing method is called Simple Exponential Smoothing (SES) (in some books, it is called “single exponential smoothing”). It can be viewed either as an adaptive-forecasting algorithm. Exponential smoothing is implemented to predict a time series with no linear trend and seasonal pattern. The observation of the short-range time series has an aperiodic variation and fluctuates around a stable mean over time. The equation for this method is as follows:
The YT and ET are the observed and forecasted value of the series at time T, and α is the smoothing constant. The above equation shows that the method constructs a weighted average of the observations [11, 12, 13], introducing single-exponential smoothing as a modern time-series method. It can produce optimal forecasts for several underlying models, including ARIMA (0,1,1) and the random-walk-plus-noise and state-space models [13].
The procedures of the Single Exponential Smoothing Method (SESM) are presented as per below:
Step 1: Compute the initial estimate of the series at period t=0.
There is no theoretical justification for estimating the initial values. It is common to calculate initial estimates of exponential smoothing procedures using historical data; however, it is not applicable in all situations. Setting it to Y1 is a method of initialization. The average of the first four or 5 observations could be another possible way of initialization.
Step 2: Compute the updated estimate using the smoothing equation.
The smoothing parameter or smoothing constant that takes values between zero and one. Note that:
The coefficients measuring the contributions of the observations decrease exponentially over time. The smoothing parameter controls the trade-off between the closeness of smoothed data to the observed data.
Although there is no generally accepted statistical procedure for choosing α, a small value for α., i.e., close to 0, has a greater smoothing effect and weighs the more distant past observations. In contrast, the value of close to one gives more weight to the recent observations. As a great suggestion to choose α, the value that made smaller Root Mean Square Error (RMSE) of the forecast, the square root of squared deviations between the forecasts and the
realized values could be a proper selection. Eventually, we used the Augmented Dickey-Fuller test for unit root to find the stationary of the data. All analysis was done by Stata12 software.
The simple exponential smoother is a special case of a simple moving average. In the moving average, all data points are assigned equal weights. Arguably, recent observation provides more relevant information than the observation in the past. Therefore, the exponential-smoothing method can give larger weights to more recent observations, and weight decreases exponentially as the observation becomes more distant. This method is more effective when the observations change slowly over time. The simple exponential smoothing method is used for short-range forecasting, usually just one lag into the future.
Results
In total, 2676 patients with MS were registered in the Khuzestan Multiple Sclerosis Center from its establishment (2006) until the end of December 2019, i.e., included in the study. The mean and SD score for the MS patients’ age was 31.40 and 8.94 years. The youngest and oldest patients were 10 and 75 years old, respectively. The sex ratio (female to male) was 3.05, meaning that one-third of the patients were male. The mean±SD age of incidence of MS was 29.19±9.16 years. Overall, 75% of patients were under 35 years of age at diagnosis. The majority had post-diploma and bachelor’s degrees (35.10%), were married (62.10%), and concerning ethnicity, were Lor (34.50%). In terms of the type of MS, RRMS was the most common type among the patients (76.3%); however, only 3.5% had the PPMS type, and 4.9% had the SPMS type (Table 1). Other details are presented in Table 1.
Table 2 shows the number of patients with MS and the total population by gender in different years of the study.
Overall, the prevalence and average annual incidence of MS disease were 57.77 and 4.35 per 100000 individuals from 2006 to 2019, respectively.
The estimated incidence and prevalence rate per 100000 individuals are displayed in Table 3.
We used the single exponential smoothing method to consider these time series data and forecast appropriately. In this regard, to have a minimum Root Mean Square Error (RMSE) for incidence and prevalence rate, the smoothing constant α is equal to 0.75 and 0.9, respectively. The first observation was used as the initial value. The trend of incidence and prevalence rate in total population, females, and males are shown in Table 3 and Figures 2 and 3. The forecasting of incidence and prevalence rate in 2020 is reported in Table 3. The study used the Augmented Dickey-Fuller test for unit root to check the linear trend and find the data’s stationery. The data for incidence had stationary in all categories. For prevalence data, the unit root test shows no stationary, i.e., attributed to the increasing nature of this data type.
The trend of incidence rate changes in Figure 2 represents that the incidence rate in females is higher than males in all years.
However, these rates get closer at the beginning of 2006, in the middle at the end of 2013, and 2019. We predict that the incidence rate in 2020 will be more or less similar to 2019 in total and for both generations.
The trend of incidence rate changes in Figure 2 represents that the incidence rate in females is higher than males in all years. However, these rates get closer at the beginning in 2006, in the middle in 2013, and at the end in 2019.
The prevalence rate changes in Figure 3 represent that multiple sclerosis is more prevalent in males.
The graph shows that the prevalence rate gets more over time. However, the increasing slope is higher for women. Our forecast for the prevalence is the same for 2020 compared to 2019.
MS, from 2006 to 2019, is more prevalent in individuals aged between twenty to fifty years old in Khuzestan province. The new cases and total populations in a 3-age category are displayed in Table 4.
The estimated incidence and prevalence rate per 100000 individuals for the three-age categories are in Table 3. The single exponential smoothing method was used to consider these time series data. To minimize the MSE and properly forecast the incidence and prevalence rate, the smoothing constant α is equal to 0.7 and 0.95, respectively. The estimated smoothing values can be seen in Table 5 and Figures 4 and 5. The forecasting of incidence and prevalence rate in 2020 is reported in Table 5.
To check the linear trend and find the data’s stationery, we used the Augmented Dickey-Fuller test for unit root. It showed that the data for incidence had stationary in all categories. For prevalence data, the test of the unit root shows no stationery.
The incidence rate of MS in three age categories is represented in Figure 4.
As we consider for individuals under 20 and above 50 years old, the incidence rate of MS had increased just slightly over time and is less than 2 per 100000 individuals. In the 20 to 50 years old individuals, the incidence rate is higher and close to 8 per 100000 individuals. We forecast that the incidence rate will increase slightly in 2020 than 2019, just for the 20-50 age category.
Figure 5 represents that MS’s prevalence rate is very high for between twenty to fifty people.
It gets more over time; however, the increasing slope is much higher for individuals aged 20 to 50. The increase in the prevalence rate of MS for under 20 years of age and above 50 has a slight slope. Moreover, our forecast for the prevalence is the same for 2020 compared to 2019 in 3 age categories.
Discussion
Our results indicated that the patients’ prevalence and average annual incidence were 57.77 and 4.35 per 100000 people from 2006 to 2019, respectively. Therefore, Khuzestan has been one of the high-risk areas for MS (prevalence of >25 per 100000 subjects).
MS prevalence and incidence have been increasing over time. Meanwhile, there is a slight change in the annual incidence of MS from 5.01 per 100000 individuals in 2006 to 4.87 per 100000 subjects in 2019. The slope of the increase in all years (from 2006 to 2019) has been higher for women than men. The number of new cases and the total population of women with MS is almost three times higher than men. However, this ratio was closer in the early years (2006), in 2013, and later in 2019. The MS incidence in women and men had increased slightly from 7.14 and 2.78 per 100000 individuals in 2006 to 7.17and 2.49 per 100000 individuals in 2019, respectively.
In 2008, we observed a decrease in the incidence. One of the significant reasons for this decrease in 2008 was the occurrence of dust in Khuzestan province and consequently the migration of some patients to neighboring provinces, such as Isfahan and Shiraz. We later saw the names of these migrating patients in the MS registration canters of those cities.
Similarly, the prevalence of MS increased from 5.01 per 100000 individuals in 2006 to 57.77 per 100000 people in 2019. Meanwhile, the MS prevalence in females and males has increased from 7.14 and 2.78 per 100000 subjects in 2006 to 85.50 and 29.06 per 100000 subjects in 2019, respectively.
Prior to this study, two other studies investigated the prevalence or incidence of the disease in Khuzestan Province; however, in smaller populations and smaller areas. Radmehr et al. estimated the prevalence of MS in northern Khuzestan at 15 per 100000, with a female-to-male ratio of 2.08 to 1 [14]. In Sharafaddinzadeh’s study, which identified 696 patients with MS in Ahvaz (Khuzestan’s capital), the prevalence and incidence of MS were 16.28 and 2.20 per 100000, respectively [15]. In other regions of Iran, in Asmarian’s study conducted on 5468 patients with MS in Fars Province, the incidence significantly increased from 1991 and 2016. At the beginning of the study (1991), the incidence rate was 0.61, and at the end (2016), it was 11.20 per 100000 individuals, and this ratio was higher in women than men in all years studied [16]. A study aimed at estimating the prevalence and incidence of MS in the Persian Gulf region, which reviewed 39 articles published from January 1985 to December 2018 in this region, reported the average age of patients with MS as 23.11 years. The disease incidence was estimated at 5.03 per 100000 and the prevalence at 39.31 per 100000, increasing by 2.3% from 1985 to 2018 [17]. In other parts of the world, the results of a study by Patti et al. in Biancavilla, Sicily, southern Italy, suggested an increase in the average annual incidence for the period 2012-2018 (16.8 per 100000 individuals), compared to the period 1992-1996 (4.5 in 100000 subjects). As of December 31, 2018, the prevalence of the disease was 292.3 per 100000 individuals (198.2 for men & 380.7 per 100000 for women), indicating a high-risk area for MS [18]. In Brola et al.’s study in Swietokrzyskie Province (central Poland), the results were similar. The prevalence of MS on December 31, 2015, was 121.3 per 100,000 people (167.1 per 100000 women, 73.2 per 100,000 men) and the average annual incidence of MS between 2010 and 2015 was about 4.5 per 100000 individuals. This rate was estimated to be much higher than in 2010 and previous studies in Poland [19].
Concerning the MS incidence in the three age groups in the present study, for individuals under 20 and over 50 years, the incidence over time has been constant and less than 2 per 100000 subjects. While in the age group of 20 to 50 years, the incidence rate was higher and close to 8 per 100000 individuals. Our age-wise results indicated a mean age of 31.40 years for patients with MS. Moreover, 75% of patients were below 35 years of age at diagnosis.
In other studies, the prevalence and incidence at a young age have been reported more than in other age groups. In Hosseinzadeh study in Iran, the mean age of patients with MS for men and women was 31.3 and 32.3 years, respectively [6]. In Cheraghmakani’s study in Mazandaran, Iran, the highest MS incidence rate is reported among the 30-34-year-old age group (28.5 per 100000 subjects), while the lowest rate was reported for above 65-year olds (0.2 per 100000 individuals) [20]. However, in Rotstein’s study, the MS prevalence increased mainly for individuals aged 35 years and older, especially individuals over 50 years [21].
Regarding some demographic and clinical variables, including the higher MS prevalence in women and the youth and the higher prevalence of relapsing-remitting MS, the results of this study are consistent with other studies.
Another variable focused in this study was the racial-ethnic aspect of patients with MS. In this study, most individuals with MS were Lors (34.5%), Persians (33.3%), and Arabs (26.3%). In this regard, Sharafaddinzadeh’s study on the impact of Persian and Arab ethnics living in Khuzestan Province on MS it was shown that the prevalence and incidence of MS were higher in the Persian population. However, the progressive nature of MS with motor symptoms and cerebellar involvement was more common in the Arab population [15]. In our study, ocular and sensory disturbances were reported as the first MS symptom more than other symptoms. Some other studies have emphasized this [15, 22]. The relationship between occupation and MS prevalence rate survey reported the highest frequency for homemakers. This is because housewives are more than working women in Iran. The MS prevalence in people with “diplomas” and “post-diploma and bachelor” has been higher than others, indicating the dominant population of Iranian society with this level of education.
Most studies evaluated the prevalence and incidence and description of the temporal trends of MS, and few have predicted the prevalence and incidence of MS in the coming years. The present study predicted that the incidence of MS in 2020 will be more or less the same compared to 2019 and will reach 4.86 per 100000 individuals, i.e., more for women than men (7.17 & 2.47 per 100000 individuals, respectively), and only in the 20-50-year-old age group. However, it is predicted that the prevalence of MS in 2020 for all age and sex groups will be more or less the same as in 2019. In this regard, in Canada, Nana et al. reviewed and presented a prognosis model over 20 years and estimated that MS cases will increase from 4051 in 2011 to 4794 in 2031. The prevalence of MS will exceed 400 per 100000 and is 3 times more common in women than in men [9]. Likewise, in Mousavizadeh’s study in Kohgiluyeh and Boyer-Ahmad, Iran, on 421 patients between 1990 and 2016, the MS prevalence was estimated to be 60.14 per 100000 the average annual incidence was 3.8 per 100000 individuals. The MS incidence was projected to increase from 8.5 per 100000 at the end of 2016 to more than 17 per 100000 individuals in 2025, and in 2025 MS will exceed 1,250, representing a nearly threefold increase in the diagnosed cases over 10 years [8].
Several factors may increase the prevalence and incidence of MS in the region between 2006 and 2019. Despite its sunny weather, vitamin D deficiency remains among the most critical health issues in Khuzestan Province [23, 24]. Further epidemiological studies have shown that serum vitamin D deficiency can be a potential environmental predisposing factor for MS in Iran [25]. Furthermore, this area’s inhabitants encounter dust particles and high temperatures. The adverse effect of Particulate Matter of 10 (PM10) on dusty days on people’s health in Ahvaz is more than days without dust [26]. A positive association between exposure to air pollution and multiple sclerosis has been reported in some studies [27, 28, 29, 30]. Lifestyle changes, increasing urbanization, and industrialization of cities can be other factors [31]. According to studies, provinces with less urbanization, such as Sistan-Baluchestan and South Khorasan in Iran, have the lowest prevalence of MS. In contrast, provinces with high urbanization, such as Tehran and Isfahan, have the highest prevalence [32].
This study has its strengths and limitations. The first study presented the prevalence and incidence of MS and presented a predictive model in all of Khuzestan Province. On the other hand, the actual number of individuals with MS may not be identified for various reasons, as follows: The elderly with long-term illness, primarily secondary progressive MS, are few. There are problems in accessing people who rarely communicate with medical services or have difficulty communicating with a physician. In addition, some young patients with mild forms of MS might avoid contacting medical services or do not require medical treatment during the study years.
Conclusion
Khuzestan Province is a high-risk area for MS. In the province, the overall prevalence has increased from 2006 to 2019. The overall incidence has been increasing with a very slight slope. The increase in prevalence and incidence was more noticeable in women than in men. The present study also predicts an increase in the incidence of MS in the coming years in the age group of 20 to 50 years. However, MS prevalence is similar to 2019. Establishing a national registry for comprehensive long-term follow-up studies is recommended.
Ethical Considerations
Compliance with ethical guidelines
The proposal of this study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (Code: IR.AJUMS.REC.1397.640).
Funding
This study was funded and supported by Ahvaz Jundishapur University of Medical Sciences (Grant No: PHT-9727).
Authors contributions
Conceptualization, methodology, supervision and project administration: Maryam Dastoorpoor; Investigation: Nastaran Majdinasab and Majid Soltani; Writing – original draft: Narges Khodadadi; Writing – review & editing: Narges Khodadadi and Maryam Dastoorpoor; Formal analysis and software: Saeed Ghanbari and Maryam Dastoorpoor.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgements
The authors wish to express their gratitude to Ms. Maryam Nedamat for her kind assistance.
Refrences
- Poser CM, Brinar VV. The accuracy of prevalence rates of multiple sclerosis: A critical review. Neuroepidemiology. 2007; 29(3-4):150-5. [DOI:10.1159/000111576] [PMID]
- The Multiple Sclerosis International Federation. Atlas of MS. London: The Multiple Sclerosis International; 2020. https://mssociety.ca/library/document/jmhzOwXi5b7erFM6nTURg4dDHWqBEao0/original.pdf
- Etemadifar M, Izadi S, Nikseresht A, Sharifian M, Sahraian MA, Nasr Z. Estimated prevalence and incidence of multiple sclerosis in Iran. Eur Neurol. 2014; 72(5-6):370-4. [DOI:10.1159/000365846] [PMID]
- Azami M, YektaKooshali MH, Shohani M, Khorshidi A, Mahmudi L. Epidemiology of multiple sclerosis in Iran: A systematic review and meta-analysis. PloS One. 2019; 14(4):e0214738. [DOI:10.1371/journal.pone.0214738] [PMID] [PMCID]
- Sahraian MA, Sahebkar M, Dehghani R, Derakhshan-Jazari M, Kazami-Moghaddam V, Kouchaki E. Multiple sclerosis-A disease on a dramatically rising trend in Iran: Review of possible reasons. Iran J Neurol. 2017; 16(1):34-40. [PMID]
- Hosseinzadeh A, Baneshi MR, Sedighi B, Kermanchi J, Haghdoost AA. Incidence of multiple sclerosis in Iran: A nationwide, population-based study. Public Health. 2019; 175:138-44. [DOI:10.1016/j.puhe.2019.07.013] [PMID]
- Jahanbani-Ardakani H, Abtahi SH, Manavi SP, Fereidan-Esfahani M. updated systematic review on epidemiology of multiple sclerosis in Iran: Central accumulation and possible role for industrial pollution. J Rev Med Sci. 2021; 1(1):16-24. http://jrevmeds.com/index.php/jrms/article/view/7
- Mousavizadeh A, Dastoorpoor M, Naimi E, Dohrabpour K. Time-trend analysis and developing a forecasting model for the prevalence of multiple sclerosis in Kohgiluyeh and Boyer-Ahmad Province, southwest of Iran. Public Health. 2018; 154:14-23. [DOI:10.1016/j.puhe.2017.10.003] [PMID]
- Amankwah N, Marrie RA, Bancej C, Garner R, Manuel DG, Wall R, et al. Multiple sclerosis in Canada 2011 to 2031: Results of a microsimulation modelling study of epidemiological and economic impacts. Health Promot Chronic Dis Prev Can. 2017; 37(2):37-48. [DOI:10.24095/hpcdp.37.2.02] [PMID] [PMCID]
- Statistical Centr of Iran. [Data on the 2016 census (Persian)]: Tehran: Statistical Centr of Iran. https://www.amar.org.ir/
- Reinsel GC. Statistical methods for forecasting. By Bovas Abraham and Johannes Ledolter. John Wiley and Sons, Inc., New York, 1983. xv + 445 pp. U.S. $38.95. ISBN 0–471–86764–0. Can J Stat. 1987; 15(3):299-300. [DOI:10.2307/3314920]
- Bowerman BL, O’Connell R, Koehler AB. Forecasting, time series, and regression (with CD-ROM)(forecasting, time series, & regression). Tyrone: South-Western College Pub; 2004. https://www.gettextbooks.com/isbn_9780534409777.html
- Chatfield C. the analysis of time series: An introduction. Florida: CRC Press; 2003. https://www.google.com/books/edition/The_Analysis_of_Time_Series/qKzyAbdaDFAC?hl=en&gbpv=0
- Radmehr M, Meghdadi S, Bahmanzadeh M, Sabbagh S. Prevalence, demographics and clinical characteristics of multiple sclerosis in North of Khuzestan Province, Iran. Jentashapir J Cell Mol Biol. 2015; 6(5):1-7. https://www.sid.ir/en/Journal/ViewPaper.aspx?ID=507230
- Sharafaddinzadeh N, Moghtaderi A, Majdinasab N, Dahmardeh M, Kashipazha D, Shalbafan B. The influence of ethnicity on the characteristics of multiple sclerosis: A local population study between Persians and Arabs. Clin Neurol Neurosurg. 2013; 115(8):1271-5. [DOI:10.1016/j.clineuro.2012.11.027] [PMID]
- Asmarian N, Sharafi Z, Mousavi A, Jacques R, Tamayo I, Bind MA, et al. Multiple Sclerosis incidence rate in southern Iran: A Bayesian epidemiological study. BMC Neurol. 2021; 21(1):309. [DOI:10.21203/rs.3.rs-34188/v1] [PMID]
- Etemadifar M, Nikanpour Y, Neshatfar A, Mansourian M, Fitzgerald S. Incidence and prevalence of multiple sclerosis in Persian Gulf area: A systematic review and meta-analysis. Mult Scler Relat Disord. 2020; 40:101959. [DOI:10.1016/j.msard.2020.101959] [PMID]
- Patti F, Caserta C, Colandonio S, Iudica ML, Maimone D, Lo Fermo S, et al. Prevalence and incidence of multiple sclerosis in the city of Biancavilla. Neuroepidemiology. 2019; 53(1-2):108-14. [DOI:10.1159/000500600] [PMID]
- Brola W, Sobolewski P, Flaga S, Fudala M, Jantarski K. Increasing prevalence and incidence of multiple sclerosis in Poland. Neurol Neurochir Pol. 2017; 51(1):82-5. [DOI:10.1016/j.pjnns.2016.11.005] [PMID]
- Cheraghmakani H, Baghbanian SM, HabibiSaravi R, Azar A, Ghasemihamedani F. Age and sex-adjusted incidence and yearly prevalence of multiple sclerosis (MS) in Mazandaran province, Iran: An 11-years study. Plos One. 2020; 15(7):e0235562. [DOI:10.1371/journal.pone.0235562] [PMID] [PMCID]
- Rotstein DL, Chen H, Wilton AS, Kwong JC, Marrie RA, Gozdyra P, et al. Temporal trends in multiple sclerosis prevalence and incidence in a large population. Neurology. 2018; 90(16):e1435-41. [DOI:10.1212/WNL.0000000000005331] [PMID]
- Kale N. Optic neuritis as an early sign of multiple sclerosis. Eye Brain. 2016; 8:195-202. [DOI:10.2147/EB.S54131] [PMID] [PMCID]
- Shojaei Shahrokhabadi M, Abbasnezhad A, Kazemnejad A, Ghaheri A, Zayeri F. Dietary intake of vitamin D pattern and its sociodemographic determinants in the southwest of Iran, Khuzestan: An application of marginalised two-part model. Adv Hum Biol. 2019; 9(3):210-5. [DOI:10.4103/AIHB.AIHB_5_19]
- Mohammadi A, Mousavi R, Afsharmanesh M, Ayashi S, Abdveys N, Kheirollah A. [Prevalence of vitamin D deficiency in patients referred to clinical diagnostic laboratories in Khuzestan Province in 2014 (Persian)]. Jundishapur Sci Med J. 2016;15(1):63-71. https://www.sid.ir/fa/journal/ViewPaper.aspx?id=287642
- Shaygannejad V, Golabchi K, Haghighi S, Dehghan H, Moshayedi A. A comparative study of 25 (OH) vitamin D serum levels in patients with multiple sclerosis and control group in Isfahan, Iran. Int J Prev Med. 2010; 1(3):195-201. [PMID]
- Shahsavani A, Tobías A, Querol X, Stafoggia M, Abdolshahnejad M, Mayvaneh F, et al. Short-term effects of particulate matter during desert and non-desert dust days on mortality in Iran. Environ Int. 2020; 134:105299. [DOI:10.1016/j.envint.2019.105299] [PMID]
- Angelici L, Piola M, Cavalleri T, Randi G, Cortini F, Bergamaschi R, et al. Effects of particulate matter exposure on multiple sclerosis hospital admission in Lombardy region, Italy. Environ Res. 2016; 145:68-73. [DOI:10.1016/j.envres.2015.11.017] [PMID] [PMCID]
- Heydarpour P, Amini H, Khoshkish S, Seidkhani H, Sahraian MA, Yunesian M. Potential impact of air pollution on multiple sclerosis in Tehran, Iran. Neuroepidemiology. 2014; 43(3-4):233-8. [DOI:10.1159/000368553] [PMID]
- Ashtari F, Esmaeil N, Mansourian M, Poursafa P, Mirmosayyeb O, Barzegar M, et al. An 8-year study of people with multiple sclerosis in Isfahan, Iran: Association between environmental air pollutants and severity of disease. J Neuroimmunol. 2018; 319:106-11. [DOI:10.1016/j.jneuroim.2018.02.019] [PMID]
- Oikonen M, Laaksonen M, Laippala P, Oksaranta O, Lilius EM, Lindgren S, et al. Ambient air quality and occurrence of multiple sclerosis relapse. Neuroepidemiology. 2003; 22(1):95-9. [DOI:10.1159/000067108] [PMID]
- Kotzamani D, Panou T, Mastorodemos V, Tzagournissakis M, Nikolakaki H, Spanaki C, et al. Rising incidence of multiple sclerosis in females associated with urbanization. Neurology. 2012; 78(22):1728-35. [DOI:10.1212/WNL.0b013e31825830a9] [PMID]
- Zarghami A, Masoud Hojjati SM. Urbanization theory for growing trend of multiple sclerosis prevalence among Iranian population. Iran J Public Health. 2016; 45(7):968-9. [PMID]
Type of Study: Research |
Subject:
Special
Received: 2022/04/6 | Accepted: 2022/04/21 | Published: 2022/04/21
Received: 2022/04/6 | Accepted: 2022/04/21 | Published: 2022/04/21
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
