Thu, Apr 25, 2024
Volume 6, Issue 1 (Winter 2020)
Caspian J Neurol Sci 2020, 6(1): 45-56 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Saghebi Saeedi K, Abolghasemi A, Akbary B. The Effectiveness of Positive Thinking and Self-compassion Training on Cognitive Flexibility and Cognitive Failure in Girls With Primary Dysmenorrhea. Caspian J Neurol Sci 2020; 6 (1) :45-56
URL: http://cjns.gums.ac.ir/article-1-305-en.html
URL: http://cjns.gums.ac.ir/article-1-305-en.html



1- Department of Psychology, Faculty of Humanities, Rasht Branch, Islamic Azad University, Rasht, Iran
2- Department of Psychology, Faculty of Humanities, University of Guilan, Rasht, Iran , abolghasemi_44@yahoo.com
2- Department of Psychology, Faculty of Humanities, University of Guilan, Rasht, Iran , abolghasemi_44@yahoo.com
Full-Text [PDF 1696 kb]
(1357 Downloads)
| Abstract (HTML) (2748 Views)
Full-Text: (1184 Views)
Introduction
Dysmenorrhea is the most common complaint in the field of gynecological diseases experienced by many women. Dysmenorrhea is divided into two types of primary and secondary based on the pathology. In primary dysmenorrhea, there are no underlying pathological conditions, while secondary dysmenorrhea is influenced by organ pathology such as endometriosis or infection [1]. Primary dysmenorrhea is one of the main factors impairing the quality of life and social activities of young women. It is the number one cause of absenteeism from school, work, and social activities. It can lead to a loss of time for studying, education, and work in women, especially in adolescence [2].
Besides, primary dysmenorrhea affects girls’ ability to concentrate on their lessons, their academic presence, and has both individual and social consequences. Dysmenorrhea can make a person feel afraid of starting the next menstrual period and endanger one’s mental health during menstruation and eventually may result in family disturbances [3]. On the other hand, due to the comorbidity of dysmenorrhea with many diseases, including polycystic ovary and endometriosis, failure to pay attention to dysmenorrhea can harm one’s general health and reproductive health.
The prevalence of painful menstruation varies from one community to another and is estimated between 2% to 5% in different communities [4, 5]. Many studies have shown the association between primary dysmenorrhea and psychological variables. L-Kindy and L-Bellouchi [6] and Ansal et al. [7] studies indicate that the quality of life in patients with primary dysmenorrhea is low due to limitations of exercise activities, decreased concentration in class, low ability to perform homework, loss of the classes, the limitations of social activities, and the decline in academic performance. Charu et al. reported the negative effect of dysmenorrhea on the quality of life and absence from work and school. Also, they showed a related decrease in the quality of life in the form of physical and psychological symptoms [8].
Zarradink et al., in their study, found that dysmenorrhea disrupts classroom focus, sleep, homework, and social relationships [9]. Also in other studies, the most common effects of dysmenorrhea on everyday life were decreased ability to concentrate and reading disorder (75%), change in physical activities (60%), the decline of mental-social health (35%), sleep disorder (26%), absence from school (19%), and hospitalization (3%). Severe dysmenorrhea disrupts usual activities and decreases the quality of work and increases the absence from work and school [10].
The decline in cognitive functioning also results in a decrease in social and occupational activity. For example, a person who is incapable of focusing on or unable to remember the simplest activities cannot certainly demonstrate the speed and efficiency required to perform his or her professional duties [11]. Evidence shows a relationship between cognitive flexibility [12] and cognitive failure [13, 14] with mental health in girls with primary dysmenorrhea.
Cognitive flexibility is the ability to modify cognitive attributes in response to changing environmental stimuli. It includes skills such as changing the perspective toward new environmental demands or conditions [15].
Ionescu answers the question of when a cognitive system is flexible as “when the ability is well adjusted to changing demands” [16]. Therefore, cognitive flexibility means that the individual is aware of his or her choices, can adapt to new situations, and feels competent in these new situations. Several studies have confirmed the relationship between cognitive flexibility and different disorders [17, 18]. Also, some people found that psychological treatment affects cognitive flexibility [19-24].
Cognitive failure is defined as the inability to finish the tasks that are usually being done. Those tasks are related to memory, inadvertent errors, and lack of recall [25] and are caused by the problems in memory, attention, and performance [13]. Cognitive failure has been investigated in several mental disorders. Body functions such as nervous system activity are associated with psychological factors in diseases. The deterioration of cognitive function, which is a hidden disease itself, causes anxiety and depression [26]. Besides, various studies have examined the effect of psychology training on cognitive failure [27-38].
Much research has been conducted on the treatment of dysmenorrhea. In many of these studies, hormonal therapies have been investigated, like increasing the number of contraceptives pills [39]. Still, hormonal pills have side effects, and some people cannot use them. Non-pharmacological treatment methods of dysmenorrhea, such as acupressure and acupuncture, muscle relaxation, magnetotherapy, reflexology, and aromatherapy, have some positive effects on reducing dysmenorrhea, but they are time-consuming and costly [40-42].
The necessity of providing a non-pharmacological treatment method for patients who do not respond to medication, suffer from side effects, or are reluctant to take the drugs is quite apparent. Non-pharmacological treatment methods make them more compatible with pain and reduce their distress, fear, and anxiety. Another benefit of these methods is to increase the effectiveness of analgesic drugs that reduce the amount of required usage [43]. One of the psychological treatments is positive thinking. Much evidence suggests that positive education interventions increase wellbeing, positive emotions, engagement, happiness, and meaning in life. Seligman presented positive psychology in the late 1990s and early 2000s [44].
Nowadays, positive psychology, as a new branch of psychology, is primarily concerned with the scientific study of human wellbeing and happiness. Nikmanesh’s research findings [45] reflect that positive psychology training provides a new way of cognitive processing and emotion regulation and reduces interpersonal and psychological problems. The key element of positive psychotherapy intervention is to educate clients to direct their attention toward positive emotions and create positive resources. The focus of positive psychology is how individuals can succeed and develop appropriate skills, abilities, and social relationships [46].
Another treatment that can alleviate dysmenorrhea is self-compassion [47]. Self-compassion is a healthy form of self-acceptance that expresses the acceptance of undesirable aspects of ourselves and our lives. According to Neff study, self-compassion involves interaction between the following three components:
1. Self-compassion (that is the tendency to have insight toward self-attention in comparison to traumatic judgments about a person).
2. Friendship versus isolation (understanding that all human beings can fail at one time, and because of this failure should not break off their relationship with others).
3. Mindfulness (the consciousness or presence of the moment) versus extreme diagnosis. The consciousness or presence of the moment is a receptive state of mind with no bias or judgment in which the individual understands his thoughts and feelings as he is, without repression or denial [47].
Self-compassion makes one feel emotionally supportive of oneself and others when faced with adversity or human defect [48]. Studies have traditionally shown that self-compassion has a positive relationship with mental health outcomes in a wide range of areas such as affect, cognitive patterns, improvement, and social achievements [49].
Sirois, in his research on chronic diseases such as bowel inflammation and arthritis, found that self-compassion improves using adaptive coping strategies, activity, and acceptance compared with incompatible styles, disaffiliation, self-blame, behavioral alienation [50]. Dunne et al. found that self-compassion training is a powerful predictor of a healthy attitude toward psychology growth, and the findings emphasized the usefulness of self-compassion education itself in promoting potential health benefits [51].
Brown et al. also found in their research that the relationship between self-compassion and wellbeing has a mediating role in attitudes towards physical change in the middle [52]. In a self-compassion and mindfulness training study to adolescents by Bluth and Eisenlohr-Moul, they found that this intervention decreases stress, depression, and anxiety symptoms and increases flexibility, appreciation, curiosity, and discovery [53].
By reviewing the literature on non-pharmacological treatment of dysmenorrhea, we found no research on the impact of being positive and self-compassion. However, some information was found on the effectiveness of other non-pharmacological treatments in dysmenorrhea. Siahpour indicated that aerobic and yoga exercises positively affects the severity, duration of pain, and the amount of analgesic drug use in patients with dysmenorrhea [54].
Reyhany research result showed that sport decreases the severity of pain in primary dysmenorrhea [55]. Jamali et al. found that exercise interventions significantly reduce pain perception indexes [56]. Farshbaf’s research results on girls with dysmenorrhea indicate that hypnotherapy and cognitive behavioral therapy are effective in reducing pain severity, and the effectiveness of hypnotherapy is more than cognitive-behavioral therapy [57].
Summary of previous research studies indicates that psychological treatments are effective in improving neuropsychological variables in patients with primary dysmenorrhea. Still, no research has been found to show the efficacy of positive psychology and self-compassion in the treatment of primary dysmenorrhea.
Regarding the prevalence of dysmenorrhea in the country (66.5% in Gilasi et al. study [4] and 40.26% in the present study), its personal and social effects [8-11], and the unwillingness of affected girls and their families to use pharmacotherapy and time-taking procedure of non-pharmacotherapy, we aimed to investigate the effectiveness of positive psychology and self-compassion training in improving neurological variables (cognitive flexibility and cognitive failure) in women with dysmenorrhea [11-14].
Materials and Methods
Research type, sample, and sampling method
This research was a quasi-experimental study with a multi-group pretest-posttest design. The effectiveness of psychological training was considered in three levels of training positive thinking, self-compassion, and lack of education (control group). The statistical population includes female high school students with primary dysmenorrhea in district one of Rasht City, Iran, in the 2017-2018 academic year. By using a multistage random cluster sampling method, 598 samples were selected among female students of the 9th to 12th grade from four schools of this district, and five classes were randomly selected from each school, and all members of that class were identified and screened.
In the next stage, the students with the primary dysmenorrhea based on menstrual symptoms scale (with scores two standard deviations above the average) were interviewed and subjects with irregular or out-of-range dysmenorrhea (21-35 days) were identified. Secondary dysmenorrhea and individuals with psychiatric disorders were excluded, and finally, 42 persons were selected through simple random sampling and placed in the experimental and control group.
In addition to justifying and expressing the research objectives, students and their parents provided their written consent to participate in the project and training courses. Before the beginning of the training, all three groups were tested and completed the questionnaires (pre-test). The duration of training of each experimental group was eight sessions (each session about 1.5 hours) that were held in the group and once weekly) like some non-pharmacological treatments). After completing the training courses, both experimental and control groups received a posttest, and the students completed the questionnaires again.
Dysmenorrhea is the most common complaint in the field of gynecological diseases experienced by many women. Dysmenorrhea is divided into two types of primary and secondary based on the pathology. In primary dysmenorrhea, there are no underlying pathological conditions, while secondary dysmenorrhea is influenced by organ pathology such as endometriosis or infection [1]. Primary dysmenorrhea is one of the main factors impairing the quality of life and social activities of young women. It is the number one cause of absenteeism from school, work, and social activities. It can lead to a loss of time for studying, education, and work in women, especially in adolescence [2].
Besides, primary dysmenorrhea affects girls’ ability to concentrate on their lessons, their academic presence, and has both individual and social consequences. Dysmenorrhea can make a person feel afraid of starting the next menstrual period and endanger one’s mental health during menstruation and eventually may result in family disturbances [3]. On the other hand, due to the comorbidity of dysmenorrhea with many diseases, including polycystic ovary and endometriosis, failure to pay attention to dysmenorrhea can harm one’s general health and reproductive health.
The prevalence of painful menstruation varies from one community to another and is estimated between 2% to 5% in different communities [4, 5]. Many studies have shown the association between primary dysmenorrhea and psychological variables. L-Kindy and L-Bellouchi [6] and Ansal et al. [7] studies indicate that the quality of life in patients with primary dysmenorrhea is low due to limitations of exercise activities, decreased concentration in class, low ability to perform homework, loss of the classes, the limitations of social activities, and the decline in academic performance. Charu et al. reported the negative effect of dysmenorrhea on the quality of life and absence from work and school. Also, they showed a related decrease in the quality of life in the form of physical and psychological symptoms [8].
Zarradink et al., in their study, found that dysmenorrhea disrupts classroom focus, sleep, homework, and social relationships [9]. Also in other studies, the most common effects of dysmenorrhea on everyday life were decreased ability to concentrate and reading disorder (75%), change in physical activities (60%), the decline of mental-social health (35%), sleep disorder (26%), absence from school (19%), and hospitalization (3%). Severe dysmenorrhea disrupts usual activities and decreases the quality of work and increases the absence from work and school [10].
The decline in cognitive functioning also results in a decrease in social and occupational activity. For example, a person who is incapable of focusing on or unable to remember the simplest activities cannot certainly demonstrate the speed and efficiency required to perform his or her professional duties [11]. Evidence shows a relationship between cognitive flexibility [12] and cognitive failure [13, 14] with mental health in girls with primary dysmenorrhea.
Cognitive flexibility is the ability to modify cognitive attributes in response to changing environmental stimuli. It includes skills such as changing the perspective toward new environmental demands or conditions [15].
Ionescu answers the question of when a cognitive system is flexible as “when the ability is well adjusted to changing demands” [16]. Therefore, cognitive flexibility means that the individual is aware of his or her choices, can adapt to new situations, and feels competent in these new situations. Several studies have confirmed the relationship between cognitive flexibility and different disorders [17, 18]. Also, some people found that psychological treatment affects cognitive flexibility [19-24].
Cognitive failure is defined as the inability to finish the tasks that are usually being done. Those tasks are related to memory, inadvertent errors, and lack of recall [25] and are caused by the problems in memory, attention, and performance [13]. Cognitive failure has been investigated in several mental disorders. Body functions such as nervous system activity are associated with psychological factors in diseases. The deterioration of cognitive function, which is a hidden disease itself, causes anxiety and depression [26]. Besides, various studies have examined the effect of psychology training on cognitive failure [27-38].
Much research has been conducted on the treatment of dysmenorrhea. In many of these studies, hormonal therapies have been investigated, like increasing the number of contraceptives pills [39]. Still, hormonal pills have side effects, and some people cannot use them. Non-pharmacological treatment methods of dysmenorrhea, such as acupressure and acupuncture, muscle relaxation, magnetotherapy, reflexology, and aromatherapy, have some positive effects on reducing dysmenorrhea, but they are time-consuming and costly [40-42].
The necessity of providing a non-pharmacological treatment method for patients who do not respond to medication, suffer from side effects, or are reluctant to take the drugs is quite apparent. Non-pharmacological treatment methods make them more compatible with pain and reduce their distress, fear, and anxiety. Another benefit of these methods is to increase the effectiveness of analgesic drugs that reduce the amount of required usage [43]. One of the psychological treatments is positive thinking. Much evidence suggests that positive education interventions increase wellbeing, positive emotions, engagement, happiness, and meaning in life. Seligman presented positive psychology in the late 1990s and early 2000s [44].
Nowadays, positive psychology, as a new branch of psychology, is primarily concerned with the scientific study of human wellbeing and happiness. Nikmanesh’s research findings [45] reflect that positive psychology training provides a new way of cognitive processing and emotion regulation and reduces interpersonal and psychological problems. The key element of positive psychotherapy intervention is to educate clients to direct their attention toward positive emotions and create positive resources. The focus of positive psychology is how individuals can succeed and develop appropriate skills, abilities, and social relationships [46].
Another treatment that can alleviate dysmenorrhea is self-compassion [47]. Self-compassion is a healthy form of self-acceptance that expresses the acceptance of undesirable aspects of ourselves and our lives. According to Neff study, self-compassion involves interaction between the following three components:
1. Self-compassion (that is the tendency to have insight toward self-attention in comparison to traumatic judgments about a person).
2. Friendship versus isolation (understanding that all human beings can fail at one time, and because of this failure should not break off their relationship with others).
3. Mindfulness (the consciousness or presence of the moment) versus extreme diagnosis. The consciousness or presence of the moment is a receptive state of mind with no bias or judgment in which the individual understands his thoughts and feelings as he is, without repression or denial [47].
Self-compassion makes one feel emotionally supportive of oneself and others when faced with adversity or human defect [48]. Studies have traditionally shown that self-compassion has a positive relationship with mental health outcomes in a wide range of areas such as affect, cognitive patterns, improvement, and social achievements [49].
Sirois, in his research on chronic diseases such as bowel inflammation and arthritis, found that self-compassion improves using adaptive coping strategies, activity, and acceptance compared with incompatible styles, disaffiliation, self-blame, behavioral alienation [50]. Dunne et al. found that self-compassion training is a powerful predictor of a healthy attitude toward psychology growth, and the findings emphasized the usefulness of self-compassion education itself in promoting potential health benefits [51].
Brown et al. also found in their research that the relationship between self-compassion and wellbeing has a mediating role in attitudes towards physical change in the middle [52]. In a self-compassion and mindfulness training study to adolescents by Bluth and Eisenlohr-Moul, they found that this intervention decreases stress, depression, and anxiety symptoms and increases flexibility, appreciation, curiosity, and discovery [53].
By reviewing the literature on non-pharmacological treatment of dysmenorrhea, we found no research on the impact of being positive and self-compassion. However, some information was found on the effectiveness of other non-pharmacological treatments in dysmenorrhea. Siahpour indicated that aerobic and yoga exercises positively affects the severity, duration of pain, and the amount of analgesic drug use in patients with dysmenorrhea [54].
Reyhany research result showed that sport decreases the severity of pain in primary dysmenorrhea [55]. Jamali et al. found that exercise interventions significantly reduce pain perception indexes [56]. Farshbaf’s research results on girls with dysmenorrhea indicate that hypnotherapy and cognitive behavioral therapy are effective in reducing pain severity, and the effectiveness of hypnotherapy is more than cognitive-behavioral therapy [57].
Summary of previous research studies indicates that psychological treatments are effective in improving neuropsychological variables in patients with primary dysmenorrhea. Still, no research has been found to show the efficacy of positive psychology and self-compassion in the treatment of primary dysmenorrhea.
Regarding the prevalence of dysmenorrhea in the country (66.5% in Gilasi et al. study [4] and 40.26% in the present study), its personal and social effects [8-11], and the unwillingness of affected girls and their families to use pharmacotherapy and time-taking procedure of non-pharmacotherapy, we aimed to investigate the effectiveness of positive psychology and self-compassion training in improving neurological variables (cognitive flexibility and cognitive failure) in women with dysmenorrhea [11-14].
Materials and Methods
Research type, sample, and sampling method
This research was a quasi-experimental study with a multi-group pretest-posttest design. The effectiveness of psychological training was considered in three levels of training positive thinking, self-compassion, and lack of education (control group). The statistical population includes female high school students with primary dysmenorrhea in district one of Rasht City, Iran, in the 2017-2018 academic year. By using a multistage random cluster sampling method, 598 samples were selected among female students of the 9th to 12th grade from four schools of this district, and five classes were randomly selected from each school, and all members of that class were identified and screened.
In the next stage, the students with the primary dysmenorrhea based on menstrual symptoms scale (with scores two standard deviations above the average) were interviewed and subjects with irregular or out-of-range dysmenorrhea (21-35 days) were identified. Secondary dysmenorrhea and individuals with psychiatric disorders were excluded, and finally, 42 persons were selected through simple random sampling and placed in the experimental and control group.
In addition to justifying and expressing the research objectives, students and their parents provided their written consent to participate in the project and training courses. Before the beginning of the training, all three groups were tested and completed the questionnaires (pre-test). The duration of training of each experimental group was eight sessions (each session about 1.5 hours) that were held in the group and once weekly) like some non-pharmacological treatments). After completing the training courses, both experimental and control groups received a posttest, and the students completed the questionnaires again.
The inclusion criteria included girls with primary dysmenorrhea, two years passed from their first menstrual period, regular menstrual periods, 14-18 years old, and healthy from the neurological and psychology aspect. The exclusion criteria included girls with secondary dysmenorrhea, pelvic pain, and neurological or psychological disorders, using pharmacotherapy, being exposed to other psychological trainings and more than three sessions absence from the training.
Research tools
Premenstrual Symptoms Screening Tool (PSST)
This inventory consists of 19 questions to investigate premenstrual Syndrome Symptoms (PMS and PMDD) and its effect on an individual’s life. The inventory consists of 2 sections (the first section includes 14 items evaluating psychological, physical and behavioral symptoms and a second section with five questions which evaluates these symptoms on an individual’s life) and the questions are answered based on 4-point Likert-type scale (never, little, average and high). In Siyahbazi et al. study, a sample of female university students residing in Tehran university dormitories was selected randomly and evaluated for validating this tool [58].
Inventory reliability was examined by the calculation of Cronbach α coefficients. The face and content methods were used for investigating the validity of inventory. The amount of Cronbach α was achieved 0.9 in testing the reliability of this test. The amount of content validity ratio and content validity index are respectively 0.7 and 0.8 that indicates the content validity of this inventory. In this study, the cutting score is considered 31.
Cognitive Flexibility Inventory (CFI)
The inventory which has been conducted by Dennis, Vander Wal is a self-report tool that has 20 questions. Its scoring is based on a 7-point Likert-type scale [59]. The concurrent validity of this inventory was equal to the Beck Depression Inventory (BDI-II) as 0.39, and its convergent validity with Martin and Robin’s cognitive flexibility scale as 0.75.
In Iran, Shareh et al. have reported the retest reliability coefficient of the whole scale as 0.75 and the Cronbach α coefficients of the whole scale as 0.30. Also, this instrument inches factor validity, convergent validity, and concurrent validity in Iran.
Cognitive Failures Inventory
Beradbent, Cooper, Fits Jerald, and Parkez prepared cognitive failure inventory in 1982. This scale has 24 items, and the responses are rated based on a 5-point scale (from never to always). This questionnaire has four components of distraction, failures related to memory, inadvertent mistake, and forgetting to remember names. In Wallace’s study, the Cronbach α coefficient of this inventory has been found 0.96, and its validity coefficient has been reported 0.51 [60]. Abolghasemi achieved the Cronbach α coefficient of this inventory as 0.99. The correlation coefficient between this questionnaire and mental health inventory is 0.41 (P<0.001) [61].
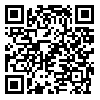
Summary of therapeutic sessions
The two protocols do not overlap because the goal of positive psychology is to transform the psychology of the individual and shift the focus from just repairing the worst to the best qualities in life. For this purpose, the flourishing of capabilities must be at the forefront of treatment and prevention (Table 1).
By teaching the components of kindness with oneself, the sense of common humanity, mindfulness refers to accepting problems as part of shared human experiences. So these problems do not occur only to specific individuals, and people are conscious of painful thoughts and feelings (mindfulness). In contrast to being absorbed completely (extreme replication) and cause fatigue and pessimism, the inefficiency of the components of burnout is reduced (Table 2).
Results
After collecting the inventories, the research data were analyzed by SPSS version 20. The mean age of the subjects was 16.52 ± 0.70 years, with the age range of 14 to 18 years.
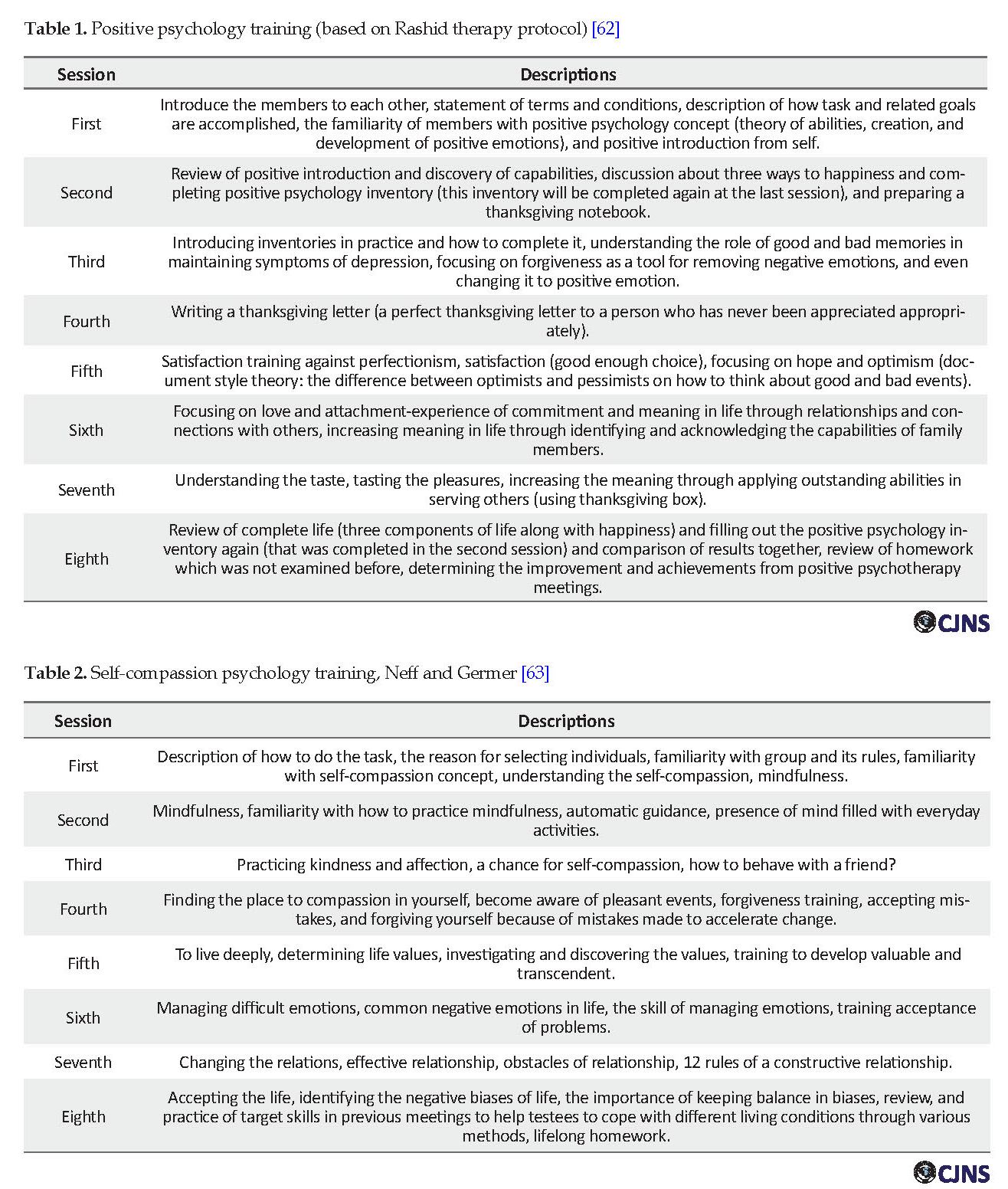
First, the Shapiro-Wilks test was used in pretest and posttest for checking the normal distribution of variables. The Shapiro-Wilks test statistic in the pretest and posttest stage is not significant for cognitive flexibility and cognitive failure, so variables distribution is normal, and we can use parametric methods such as F-test, regression slope, homogeneity of variances and Levene’s test.
Also, Table 3 presents the mean and standard deviation of cognitive flexibility and cognitive failure scores of participants.
Research tools
Premenstrual Symptoms Screening Tool (PSST)
This inventory consists of 19 questions to investigate premenstrual Syndrome Symptoms (PMS and PMDD) and its effect on an individual’s life. The inventory consists of 2 sections (the first section includes 14 items evaluating psychological, physical and behavioral symptoms and a second section with five questions which evaluates these symptoms on an individual’s life) and the questions are answered based on 4-point Likert-type scale (never, little, average and high). In Siyahbazi et al. study, a sample of female university students residing in Tehran university dormitories was selected randomly and evaluated for validating this tool [58].
Inventory reliability was examined by the calculation of Cronbach α coefficients. The face and content methods were used for investigating the validity of inventory. The amount of Cronbach α was achieved 0.9 in testing the reliability of this test. The amount of content validity ratio and content validity index are respectively 0.7 and 0.8 that indicates the content validity of this inventory. In this study, the cutting score is considered 31.
Cognitive Flexibility Inventory (CFI)
The inventory which has been conducted by Dennis, Vander Wal is a self-report tool that has 20 questions. Its scoring is based on a 7-point Likert-type scale [59]. The concurrent validity of this inventory was equal to the Beck Depression Inventory (BDI-II) as 0.39, and its convergent validity with Martin and Robin’s cognitive flexibility scale as 0.75.
In Iran, Shareh et al. have reported the retest reliability coefficient of the whole scale as 0.75 and the Cronbach α coefficients of the whole scale as 0.30. Also, this instrument inches factor validity, convergent validity, and concurrent validity in Iran.
Cognitive Failures Inventory
Beradbent, Cooper, Fits Jerald, and Parkez prepared cognitive failure inventory in 1982. This scale has 24 items, and the responses are rated based on a 5-point scale (from never to always). This questionnaire has four components of distraction, failures related to memory, inadvertent mistake, and forgetting to remember names. In Wallace’s study, the Cronbach α coefficient of this inventory has been found 0.96, and its validity coefficient has been reported 0.51 [60]. Abolghasemi achieved the Cronbach α coefficient of this inventory as 0.99. The correlation coefficient between this questionnaire and mental health inventory is 0.41 (P<0.001) [61].
Summary of therapeutic sessions
The two protocols do not overlap because the goal of positive psychology is to transform the psychology of the individual and shift the focus from just repairing the worst to the best qualities in life. For this purpose, the flourishing of capabilities must be at the forefront of treatment and prevention (Table 1).
By teaching the components of kindness with oneself, the sense of common humanity, mindfulness refers to accepting problems as part of shared human experiences. So these problems do not occur only to specific individuals, and people are conscious of painful thoughts and feelings (mindfulness). In contrast to being absorbed completely (extreme replication) and cause fatigue and pessimism, the inefficiency of the components of burnout is reduced (Table 2).
Results
After collecting the inventories, the research data were analyzed by SPSS version 20. The mean age of the subjects was 16.52 ± 0.70 years, with the age range of 14 to 18 years.
First, the Shapiro-Wilks test was used in pretest and posttest for checking the normal distribution of variables. The Shapiro-Wilks test statistic in the pretest and posttest stage is not significant for cognitive flexibility and cognitive failure, so variables distribution is normal, and we can use parametric methods such as F-test, regression slope, homogeneity of variances and Levene’s test.
Also, Table 3 presents the mean and standard deviation of cognitive flexibility and cognitive failure scores of participants.
Univariate Analysis of Covariance (ANCOVA) was used for analyzing data and responding to questions. F-test was used for examining the homogeneity assumptions of pretest and posttest regression slope, cognitive flexibility, and cognitive failure in positive psychology training groups, self- compassion, and control. F statistic is not significant (P>0.05), so the assumption of homogeneity of regression slope exists, and there is no obstacle for continuing analysis.
Levene’s test was used for comparing the variance of two groups to investigate the homogeneity of experimental and control groups in the posttest of cognitive flexibility and cognitive failure with regard to lack of significance of Levene’s statistic in cognitive flexibility (F=1.21, P>0.05) and cognitive failure (F=1.47, P>0.05), homogeneity assumption of groups exist, and there is no obstacle to analyze it.
Levene’s test was used for comparing the variance of two groups to investigate the homogeneity of experimental and control groups in the posttest of cognitive flexibility and cognitive failure with regard to lack of significance of Levene’s statistic in cognitive flexibility (F=1.21, P>0.05) and cognitive failure (F=1.47, P>0.05), homogeneity assumption of groups exist, and there is no obstacle to analyze it.
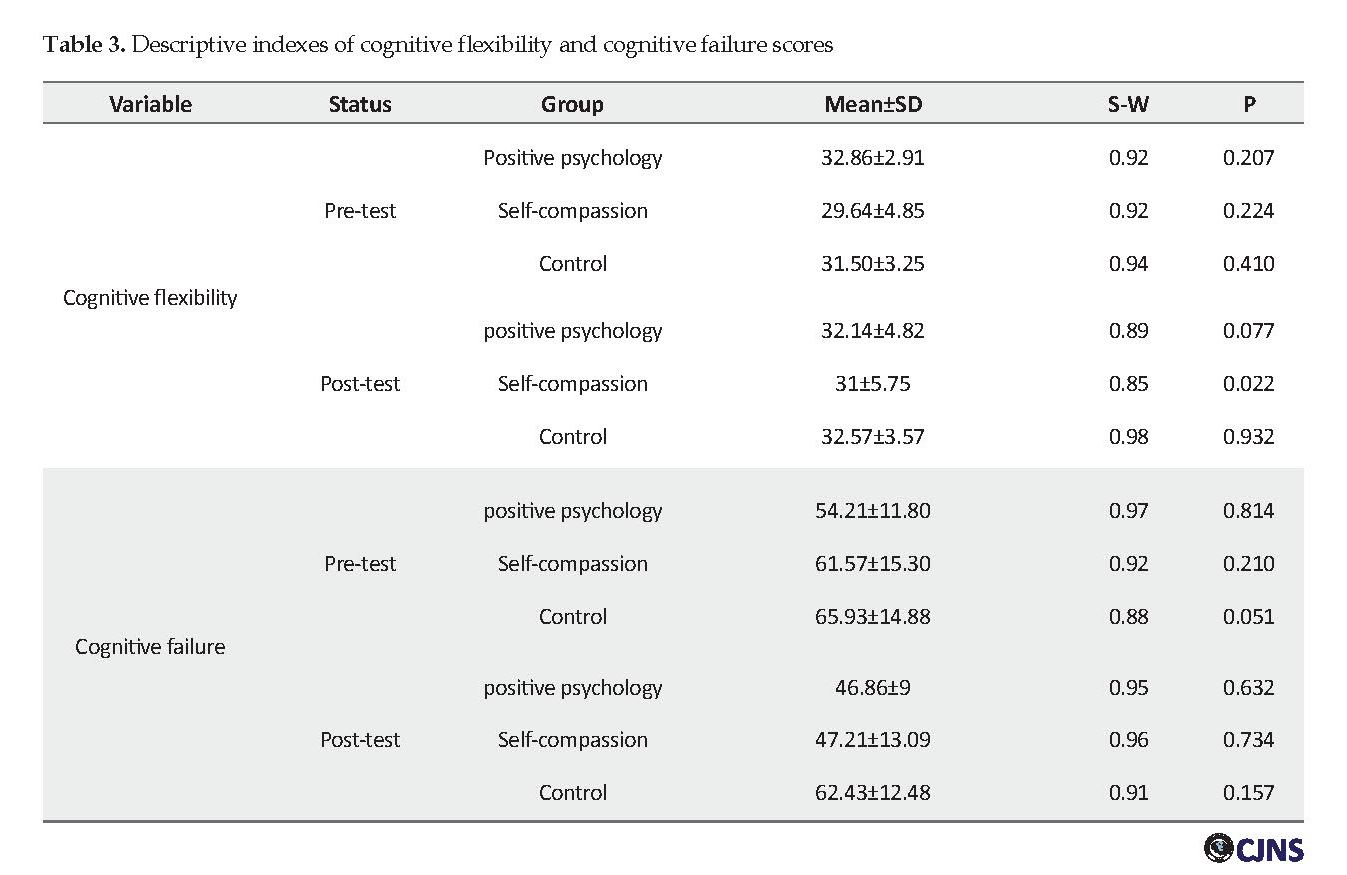
Table 4 presents the results of univariate Analysis of Covariance (ANCOVA) for examining the difference between experimental and control groups in cognitive flexibility and cognitive failure, with controlling the pretest of this variable. The results show no significant difference between the two experimental and control groups in cognitive flexibility (F=0.16, P>0.05). The results also indicate a significant difference between the three groups in cognitive failure (F=7.19, P<0.05).
Eta squared shows that the difference between the three groups in the posttest variable, regarding statistical control of pretest, is generally significant, and this difference is 0.274. It means that 27.4% of variance relating to the difference between the two groups in the posttest results from experimental conditions.
Table 5 presents adjusted cognitive failure means to investigate the mean of which group in cognitive failure posttest after adjusting pretest scores is lower. The adjusted means indicate that experimental conditions with 95% confidence have been effective in reducing the cognitive failure of students affected by dysmenorrhea.
In Table 6, Bonferroni test results indicate that self-compassion and positive psychology of experimental groups compared with the control group in the case of cognitive failure have lower scores.
Discussion
This study aimed to investigate the effectiveness of positive thinking and self-compassion training on cognitive flexibility and cognitive failure in women with primary dysmenorrhea, and the results indicated no significant difference between the three groups in cognitive flexibility (P>0.05). There is no other study that shows the effectiveness of these two training on cognitive flexibility in affected girls by dysmenorrhea.
Soltani et al. research results consistent with current research results showed that interference of mindfulness, based on reducing stress, had no significant effect on cognitive flexibility in veterance affected by this disorder [19].
In studies inconsistent with Soltani et al. [19] study, Stone and Egochi [20], Fazeli and et al. [18], Cheragh Sahar and Atashpoor [21], Abdi [22], Zare [23], Abbasi [24], different cognitive therapies were effective in improving cognitive flexibility.
The following factors could explain the difference between these results and the literature review. The subjects in this study were teenage girls affected by primary dysmenorrhea and were different from other samples in similar studies. The other factors are study settings and noisy environment (research classes of this study were held in schools), girls puberty, and its interference with social functions (these functions are subject to growth) such as selective attention and cognitive flexibility. Also, the research girls are in growing age, and their structure and performance of the brain have not reached to its final growth and finally insufficiently trained techniques and the effectiveness and interference of homework practicing these techniques at home.
The result of statistical analysis revealed that training and self-compassion training were effective in reducing cognitive failure of girls affected by primary dysmenorrhea, and there is a significant difference between three groups in cognitive failure (F=7.19, P<0.005) and self-compassion had more effect than positive psychology. There was no other study which investigates the effectiveness of these two training programs on reducing cognitive failure in patients.
However, other effective psychology training such as mindfulness, metacognition, and cognitive-behavioral training (because of having common factors with positive psychology and self-compassion) on reducing cognitive failure in different patients confirm the positive effect of these training programs on reducing cognitive failure in patients. Mir Nasab et al. [28], Abolghasemi and Kiyamarci [27], Taghavi [30], Teper and Inzlicht [31], and Asadi [34] studies consistent with the current research found the positive impact of psychological training on improving the cognitive failure.
Noguchi research consistent with the present study showed that mindfulness training could increase cognitive flexibility and reduce cognitive failure in people [35]. Along with this research, Abbariky et al. study indicate that cognitive rehabilitation program reduces cognitive failure in children with learning disorder [36].
In describing these findings, we can say that because mindfulness is a feeling of balance without judgment, which helps to accept the emotions and physical phenomena as they occur, its training causes people to accept their feelings and psychological symptoms and decrease their attention and sensitivity toward these symptoms.
Self-compassion and positive psychology as positive psychology traits are more likely to improve conditions, acceptance of abilities, and an individual’s mental wellbeing. Studies have shown that compassion-focused techniques are related to positive outcomes and can help individuals affected by mental disorders [29].
Those who have a high level of self-compassion usually benefit from self-compassion and common human sense like altruism, and this feature provides the cause of mental health and the creation of internal motivation for growth and development. Self-compassion with increasing social relationships and decreasing self-criticism reduces an individual’s rumination, thought suppression, anxiety, and mental pressure and balance. In this regard, flexibility in thoughts and self-compassion causes individuals to have realistic judgment toward themselves and analyze their performance failures and make proper decisions to solve them.
The key aspect of self-compassion therapy in patients with mental disorders include helping them to improve growth, acceptance, attention, and proper attitude toward difficult internal experiences [32]. In this case, Smeets et al. indicated that positive view toward future (as one of the positive psychology factors) is the most important benefit of self-compassion and compassion intervention in increasing the individuals’ optimism about their abilities while confronting challenging situations is effective, perhaps because this reduces self-judgment which causes to loss of competency perception [33].
To explain the more impact of self-compassion training compared with positive psychology training on improving cognitive failure, we can say that self-compassion techniques are self-centered and focus more on self-awareness and consciousness. The mindfulness reduces the person’s painful thoughts and emotions as opposed to being fully absorbed by extreme coping, memory deficits, inadvertent errors, and lack of recall of names that are components of cognitive impairment.
While focusing on positive techniques, focusing on empowerment and generating positive emotions, improving the trait of gratitude and forgiveness of others is emphasized, and, in addition to promoting positive knowledge in the individual, it improves his or her relationship with those around him or her. To point out the importance of this issue, we can refer to Narimani's study [37]. Identifying student’s strong points improves self-esteem and has a positive effect on their next performance. With reliance on psychological confidence, students can focus more on their actions and behaviors and manage them well.
Attention to human common things can create a sense of co-nature with others that prevent them from extreme judgments toward themselves, which is disruptive of appropriate performance. Reducing mental isolation provides more interaction with others and leads to acquiring various leaving experiences for individuals [37].
Individuals with high self-compassion, high self-acceptance, and low self-criticism, feel valued. Additionally, in experiencing unpleasant events that involve social evaluation and comparison, they know that all humans may make mistakes and commit wrong things, so they experience less negative feelings (human common things factors). They accept their mistakes and try to compensate instead of drowning in negative emotions and blame himself/herself, feeling lonely and being alone, so they never lose their self-esteem. Generally speaking, individuals with self-compassion are more optimistic and, therefore, can better cope with their negative emotions (as one of the positive factors). Also, training and practices which have been performed to increase self-compassion can be effective in improving different forms of disorders [38].
Conclusion
In this study, the effectiveness of positive psychology and self-compassion training on cognitive flexibility and cognitive failure were examined in girls with primary dysmenorrhea. Although self-compassion and positive psychology training did not affect cognitive flexibility, they were effective in improving girl’s cognitive failure. This study had some limitations. Some students did not cooperate in homework assignments and did not take non-pharmacological methods seriously. Also, the results cannot be generalized.
In addition, due to time limitation and lack of access to students, the follow-up stage was not performed. To achieve conclusive results, it is recommended to conduct future research in other populations with dysmenorrhea and investigate the effect in the follow-up stage.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of the Islamic Azad University of Rasht branch on September 24, 2018 (IR.IAURASHT.REC.1397.006). All the study procedures were in compliance with the ethical guidelines of the Declaration of Helsinki, 2013.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
Coceptualization, methodology: All authors; Investigation: Karameh Saghebi Saeedi; Writing-original draft: Karameh Saghebi Saeedi; Writing- review & editing: Abbas Abolghsemi, Karameh Saghebi Saeedi; Funding acquisition, resources: Karameh Saghebi Saeedi; Supervision: Abbas Abolghasemi, Bahman Akbari.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors appreciate the education officials of district one, school principals, and students who sincerely contribute to perform this study.
References
Aksu H, Özsoy S. Primary dysmenorrhea and herbals. J Health Commun. 2016; 1(23):1-3. [DOI:10.4172/2472-1654.100023]
Abaraogu UO, Tabansi-Ochuogu CS. As acupressure decreases pain, acupuncture may improve some aspects of quality of life for women with primary dysmenorrhea: A systematic review with meta-analysis. J Acupunct Meridian Stud. 2015; 8(5):220-8. [DOI:10.1016/j.jams.2015.06.010] [PMID]
Speroff L, Glass RH, Kase NG. Clinical gynecologic endocrinology and infertility. 6th ed. Baltimore: Lippincott, Williams & Wilkins; 1999.
Gilasi G, Suki Z, Kohzadi SH, Khasi B. [Investigate the prevalence of dysmenorrhea and some related factors in female students in Kashan University of Medical Sciences (Persian)]. Zanko J Med Sci. 2015: 28-34.
Ibrahim NK, AlGhamdi MS, Al-Shaibani AN, Ali-AlAmri F, Abdulrahman-Alharbi H, Al-Jadani AK, et al. Dysmenorrhea among female medical students in King Abdulaziz University: Prevalence, predictors and outcome. Pak J Med Sci. 2015; 31(6):1312-7. [DOI:10.12669/pjms.316.8752] [PMID] [PMCID]
Al-Kindi R, Al-Bulushi A. Prevalence and impact of dysmenorrhea among Omani. Sultan Qaboos Uni Medl J. 2011; 11(4):485-91.
Unsal A, Ayranci U, Tozun M, Arsalan G, Calik E. Prevalence dysmenorrhea and its effect on quality of life among a group of female university students. Upsala J Med Sci. 2010; 115:138-45. [DOI:10.3109/03009730903457218] [PMID] [PMCID]
Charu S, Amita R, Sujoy R, Thomas JA. Menstrual characteristics’ and ‘prevalence and effects of dysmenorrhea on quality of life of medical students. Int J Collab Res Intern Med Pubic Health. 2012; 4(4):276-94.
Zahradnik H-P, Hanjalic-Beck A, Groth K. Nonsteroidal anti-inflammatory drugs and hormonal contraceptives for pain relief from dysmenorrhea: A review. Contracept. 2010; 81(3):185-96. [DOI:10.1016/j.contraception.2009.09.014] [PMID]
Chen HY, Lin YH, Su IH, Chen YC, Yang SH, Chen JL. Investigation on Chinese herbal medicine for primary dysmenorrhea: Implication from a nationwide prescription database in Taiwan. Complement Ther Med. 2014; 22(1):116-25. [DOI:10.1016/j.ctim.2013.11.012] [PMID]
Sanaat Negar S, Rostami R. [Traumatic brain damage and effectiveness of cognitive rehabilitation in the improvement of attention, memory and exclusive function of affected patients (Persian)]. GenPsych. 2014; 3(7):63-80.
Gabrys RL, Tabri N, Anisman H, Matheson K. Cognitive control and flexibility in the context of stress and depressive symptoms: The cognitive control and flexibility questionnaire. Front Psychol. 2018; 9:2219. [DOI:10.3389/fpsyg.2018.02219] [PMID] [PMCID]
Unsworth N, Brewer GA, Spillers GJ. Variation in cognitive failures: An individual differences investigation of everyday attention and memory failures. J Mem Lang. 2012; 67:1-16. [DOI:10.1016/j.jml.2011.12.005]
Tirre WC. Dimensionality and determinants of self-reported cognitive failures. Int J Psychol Res. 2018; 11(1):9-18. [DOI:10.21500/20112084.3213]
Carbonella JY, Timpano KR. Examining the link between hoarding symptoms and cognitive flexibility deficits. Behav Ther. 2016; 47(2):262-73. [DOI:10.1016/j.beth.2015.11.003] [PMID]
Ionescu T. When is a cognitive system flexible? The variability-stability-flexibility pattern on the way to novel solutions. AVANT. 2017; 8:252-64. [DOI:10.26913/80s02017.0111.0023]
Meiran N, Diamond GM, Toder D, Nemets B. Cognitive rigidity in unipolar depression and obsessive compulsive disorder: Examination of task switching, stroop, working memory updating and post-conflict adaptation. Psychiatry Res. 2011; 185:149-56. [DOI:10.1016/j.psychres.2010.04.044] [PMID]
Fazeli M, Ehteshamzadeh P, Hashemi Sheikh Bahani E. [The effectiveness of cognitive behavior therapy on cognitive flexibility of depressed people (Persian)]. Thought Behav Clin Psychol. 2014; 9(34):27-36.
Soltani E, Shareh H, Bahrainian A, Farmani A. [The mediating role of cognitive flexibility in correlation of coping styles and resilience with depression (Persian)]. Pejouhandeh. 2013; 18(2):88-96.
Stone WS, Iguchi L. Stress and mental flexibility in autism spectrum disorders. N Am J Med Sci. 2013; 3(6):145-53.
Cheragh sahar Z, Atashpoor H. [The effectiveness positive cognitive-behavioural training in children mother’s cognitive flexibility affected by defeat hyperactivity disorder. Third national meeting of developing and promoting (Persian)]. Tehran, Association for the development and promotion of science and technology. 2015.
Abdi R, Chalabianloo G, Jabari G. [Effect of mindfulness practices on executive functions of elementary school students (Persian)]. Plant Cell Physiol. 2016; 4(1):9-16
Zare H. [Effectiveness of acceptance and commitment therapy (ACT) on improving the flexibility and cognitive fusion (Persian)]. Soc Cogn. 2017: 6(1):125-34.
Abbasi M, Pirani Z, Dargahi Sh, Bonyadi F. [Role of procrastination and motivational self-regulation in predicting students’ academic engagement (Persian)]. Iran J Med Educ. 2015; 15:160-9.
Abolghasemi A. [Psychological test. (Persian)]. Ardabil: Baghe Rezvan Press; 2005
Carrigan N, Barkus E. A systematic review of cognitive failures in daily life: Healthy populations. Neurosci Biobehav Rev. 2016; 63:29-42. [DOI:10.1016/j.neubiorev.2016.01.010] [PMID]
Abolghasemi A, Kiyamarei A. [The relationship between metacognition and cognitive failures in the elderly (Persian)]. Adv Cogn Sci. 2009; 11(1):8-15.
Mir Nasab MM, Mansour M, Afrouz GHA, Ghobari Bonab B, Behpaghouh A. [Impact of behavior therapy and cognitive-behavior therapy on amelioration of ADHD symptoms (Persian)]. J Except Child. 2008; 8(1):70-84.
Gilbert P. Compassion focused therapy: Special issue. Int J Cog Ther. 2010; 3(2):95-201. [DOI:10.1521/ijct.2010.3.2.95]
Taghavi Z. [Effectiveness of cognitive-behavioural therapy on reducing symptoms and increasing children self-control who have deficit hyperactivity disorder (Persian)]. [MA Thesis]. Tehran: Allame Tabatabaei University; 2010.
Teper R, Inzlicht M. Meditation, mindfulness and executive control. Soc Cog Affect Neurosci. 2013; 8(1):85-92. [DOI:10.1093/scan/nss045] [PMID] [PMCID]
Braehler C, Gumley A, Harper J, et al. Exploring change processes in compassion focused therapy in psychosis: Results of a feasibility randomized controlled trial. Br J Clin Psych 2013; 52(2):199-214. [DOI:10.1111/bjc.12009] [PMID]
Smeets E, Neff KD, Alberts H, Peters M. Meeting suffering with kindness: Effects of a brief self-compassion intervention for female college students. J Clin Psychol. 2014; 70(9):794-807. [DOI:10.1002/jclp.22076] [PMID]
Asadi S, Abolghasemi, A, Basharpoor S. [The effectiveness of mindfulness- based cognitive therapy on cognitive failure and emotional processing in anxious nurses (Persian)]. Iran J Neonatol. 2016; 29(102):55-65. [DOI:10.29252/ijn.29.102.55]
Noguchi K. Mindfulness as an end-state: Construction of a trait measure of mindfulness. Pers Individ Dif. 2017; 106:298-307. [DOI:10.1016/j.paid.2016.10.047]
Abbariky A, Yazdanbakhsh K, Momeni k. [The effectiveness of computer-based cognitive rehabilitation on reducing cognitive failure in students with learning disability (Persian)]. Q Psychol Except Individ. 2017; 7(26):127-57.
Narimani M, Einy S, Tagavy R. [Explaining students’ academic burnout based on self-compassion and sense of coherence (Persian)]. Jefferson Cent Ment Health. 2018; 5(1):36-47.
GhadamPoor E, Mansouri L. [The effectiveness of compassion-focused therapy on increasing optimism and self-sufficiency in female students with anxiety disorders (Persian)]. Gen Psychol Stud. 2018; 14(1):59-74.
Mohamed H, Neaem S. The effect of dysmenorrhea on quality of life of technical secondary schools girls. Med J Cairo Uni. 2013; 81(2):83-9.
Kannan P, Claydon LS. Some physiotherapy treatments may relieve menstrual pain in women with primary dysmenorrhea: A systematic review. J Physiother. 2014; 60(1):13-21. [DOI:10.1016/j.jphys.2013.12.003] [PMID]
She Y, Ma L, Zhu J, Qi C, Wang Y, Tang L, et al. Comparative study on skin temperature response to mensturationat acupuncture points in healthy volunteers and primary dysmenorrhea patients. J Tradit Chin Med Sci. 2017; 37(2):220-8. [DOI:10.1016/S0254-6272(17)30048-1]
Chen Chen X, Draucker Claire B, Carpente Janet S. What women say about their dysmenorrhea: A qualitative thematic analysis. BMC Womens Health. 2018; 18(47):1-17. [DOI:10.1186/s12905-018-0538-8] [PMID] [PMCID]
Ghomari Givi H, Sharei SJ, Mohammadipour Rik N, et al. [Evaluation of the effectiveness of relaxation and distraction techniques to reduce and Pain control in hospitalized children (Persian)]. Couns Psychother Cult. 2012; 3(10):101-15.
Seligman MEP, Ernst RM, Gillham J, Reivich K, Linkins, M. Positive education: Positive psychology and classroom interventions. Oxf Rev Educ. 2009; 35(3):293-311. [DOI:10.1080/03054980902934563]
Nick Manesh Z, Zandvokil M. [The effect of positive thinking training on quality of life, depression, stress and anxiety in delinquent juveniles (Persian)]. Posit Psychol Res. 2015; 1(2):53-64.
Hayes L, Ciarrochi J. The thriving adolescent: Using acceptance and commitment therapy and positive psychology to help young people manage emotions, achieve goals, and build positive relationships. Oakland. CA: Context Press; 2015.
Neff KD. Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self Identity. 2003; 2:85-102. [DOI:10.1080/15298860309032]
Yanel LM, Neff KD. Self-compassion, interpersonal conflict. Resolution, and well- being. Self Identity. 2013; 12:146-59. [DOI:10.1080/15298868.2011.649545]
Akin A, Akin U. Self-compassion as a predictor of social safeness in Turkish university students. Revista Latinoam Psicología. 2015; 47(1):43-9. [DOI:10.1016/S0120-0534(15)30005-4]
Sirois MF. A self-regulation resource model of self-compassion and health behavior intentions in emerging adults. Prev Med Rep. 2015; 2:218-22. [DOI:10.1016/j.pmedr.2015.03.006] [PMID] [PMCID]
Dunne S, Sheffield D, Chilcot J. Brief report: Self-compassion, physical health and the mediating role of health-promoting behaviours. J Health Psychol. 2018; 23(7):993-9. [DOI:10.1177/1359105316643377] [PMID]
Brown L, Bryant C, Brown, V, Bei B, Judd F. Self-compassion, attitudes to ageing and indicators of health and well-being being among midlife women. Aging & Mental Health. 2016; 20(10):1035-43. [DOI:10.1080/13607863.2015.1060946] [PMID]
Bluth K, Eisenlohr-Moul TA. Response to a mindful self-compassion intervention in teens: A within-person association of mindfulness, self-compassion, and emotional well-being outcomes. J Adolesc. 2017; 57:108-18. [DOI:10.1016/j.adolescence.2017.04.001] [PMID] [PMCID]
Siahpour T, Nikbakht M, Rahimi A, Rabiei MA. [Effect of eight weeks aerobic training and yoga on primary dysmenorrhea (Persian)]. Armaghane Danesh. 2013; 18(6):475-83.
Reyhani T, Jafarnezhad F, Hosseini B, Ajam M, Baghaei M. [Investigating the effect of fast walking on girl student’s dysmenorrhea and women infertility (Persian)]. Iran J Obstet, Gynaecol Infertil. 2013; 16(46):14-9.
Jamali F, Moazzami M, Bijan N. [The effect of eight weeks aerobic training on serum beta-endorphosis and perception of dysmenorrhea in inactive teenage girls (Persian)]. J Sabzevar Uni Med Sci 2014; 21(14):702-10.
Farshbaf Mani Sefat F, Abolghasemi A, Borhanmand O, Hajloo N. [Comparison of the effectiveness of cognitive-behavioral therapy and hypnotherapy therapy on pain self-efficacy and pain severity in girls with primary dysmenorrhea (Persian)]. Armaghane Danesh. 2017; 22(1):87-103.
Siahbazi SH, Hariri FZ, Montazeri A, Moghaddam Banaem L. [Translation and psychometric properties of the Iranian version of the Premenstrual Symptoms Screening Tool (PSST) (Persian)]. Payesh. 2011; 10(4):421-7.
Dennis JP, Vander Wal JS. The cognitive flexibility inventory: Instrument development and estimates of reliability and validity. Cognit Ther Res. 2010; 34:241-53. [DOI:10.1007/s10608-009-9276-4]
Wallace JC, Vodanovich SJ, Restino BM. Predicting cognitive failures from boredom proneness and daytime sleepiness scores: An investigation within military and undergraduate samples. Pers Individ Dif. 2003; 34:635-44. [DOI:10.1016/S0191-8869(02)00050-8]
Abolghasemi A. Investigating the relationship between metacognitive and religious beliefs with cognitive failures in older and older people. Ardabili: University of Mohaghegh Ardabili; 2007.
Rashid T. Positive psychotherapy: Exploring the best in people. In: Shane J. Lopez, editor. Positive Psychology: Pursuing Human Flourishing. Westport: Praeger; 2008.
Neff KD, Germer CK. A pilot study and randomized controlled trial of the mindful self-compassion program. J Clin Psychol. 2013; 69(1):28-44. [DOI:10.1002/jclp.21923] [PMID]
Eta squared shows that the difference between the three groups in the posttest variable, regarding statistical control of pretest, is generally significant, and this difference is 0.274. It means that 27.4% of variance relating to the difference between the two groups in the posttest results from experimental conditions.
Table 5 presents adjusted cognitive failure means to investigate the mean of which group in cognitive failure posttest after adjusting pretest scores is lower. The adjusted means indicate that experimental conditions with 95% confidence have been effective in reducing the cognitive failure of students affected by dysmenorrhea.
In Table 6, Bonferroni test results indicate that self-compassion and positive psychology of experimental groups compared with the control group in the case of cognitive failure have lower scores.
Discussion
This study aimed to investigate the effectiveness of positive thinking and self-compassion training on cognitive flexibility and cognitive failure in women with primary dysmenorrhea, and the results indicated no significant difference between the three groups in cognitive flexibility (P>0.05). There is no other study that shows the effectiveness of these two training on cognitive flexibility in affected girls by dysmenorrhea.
Soltani et al. research results consistent with current research results showed that interference of mindfulness, based on reducing stress, had no significant effect on cognitive flexibility in veterance affected by this disorder [19].
In studies inconsistent with Soltani et al. [19] study, Stone and Egochi [20], Fazeli and et al. [18], Cheragh Sahar and Atashpoor [21], Abdi [22], Zare [23], Abbasi [24], different cognitive therapies were effective in improving cognitive flexibility.
The following factors could explain the difference between these results and the literature review. The subjects in this study were teenage girls affected by primary dysmenorrhea and were different from other samples in similar studies. The other factors are study settings and noisy environment (research classes of this study were held in schools), girls puberty, and its interference with social functions (these functions are subject to growth) such as selective attention and cognitive flexibility. Also, the research girls are in growing age, and their structure and performance of the brain have not reached to its final growth and finally insufficiently trained techniques and the effectiveness and interference of homework practicing these techniques at home.
The result of statistical analysis revealed that training and self-compassion training were effective in reducing cognitive failure of girls affected by primary dysmenorrhea, and there is a significant difference between three groups in cognitive failure (F=7.19, P<0.005) and self-compassion had more effect than positive psychology. There was no other study which investigates the effectiveness of these two training programs on reducing cognitive failure in patients.
However, other effective psychology training such as mindfulness, metacognition, and cognitive-behavioral training (because of having common factors with positive psychology and self-compassion) on reducing cognitive failure in different patients confirm the positive effect of these training programs on reducing cognitive failure in patients. Mir Nasab et al. [28], Abolghasemi and Kiyamarci [27], Taghavi [30], Teper and Inzlicht [31], and Asadi [34] studies consistent with the current research found the positive impact of psychological training on improving the cognitive failure.
Noguchi research consistent with the present study showed that mindfulness training could increase cognitive flexibility and reduce cognitive failure in people [35]. Along with this research, Abbariky et al. study indicate that cognitive rehabilitation program reduces cognitive failure in children with learning disorder [36].
In describing these findings, we can say that because mindfulness is a feeling of balance without judgment, which helps to accept the emotions and physical phenomena as they occur, its training causes people to accept their feelings and psychological symptoms and decrease their attention and sensitivity toward these symptoms.
Self-compassion and positive psychology as positive psychology traits are more likely to improve conditions, acceptance of abilities, and an individual’s mental wellbeing. Studies have shown that compassion-focused techniques are related to positive outcomes and can help individuals affected by mental disorders [29].
Those who have a high level of self-compassion usually benefit from self-compassion and common human sense like altruism, and this feature provides the cause of mental health and the creation of internal motivation for growth and development. Self-compassion with increasing social relationships and decreasing self-criticism reduces an individual’s rumination, thought suppression, anxiety, and mental pressure and balance. In this regard, flexibility in thoughts and self-compassion causes individuals to have realistic judgment toward themselves and analyze their performance failures and make proper decisions to solve them.
The key aspect of self-compassion therapy in patients with mental disorders include helping them to improve growth, acceptance, attention, and proper attitude toward difficult internal experiences [32]. In this case, Smeets et al. indicated that positive view toward future (as one of the positive psychology factors) is the most important benefit of self-compassion and compassion intervention in increasing the individuals’ optimism about their abilities while confronting challenging situations is effective, perhaps because this reduces self-judgment which causes to loss of competency perception [33].
To explain the more impact of self-compassion training compared with positive psychology training on improving cognitive failure, we can say that self-compassion techniques are self-centered and focus more on self-awareness and consciousness. The mindfulness reduces the person’s painful thoughts and emotions as opposed to being fully absorbed by extreme coping, memory deficits, inadvertent errors, and lack of recall of names that are components of cognitive impairment.
While focusing on positive techniques, focusing on empowerment and generating positive emotions, improving the trait of gratitude and forgiveness of others is emphasized, and, in addition to promoting positive knowledge in the individual, it improves his or her relationship with those around him or her. To point out the importance of this issue, we can refer to Narimani's study [37]. Identifying student’s strong points improves self-esteem and has a positive effect on their next performance. With reliance on psychological confidence, students can focus more on their actions and behaviors and manage them well.
Attention to human common things can create a sense of co-nature with others that prevent them from extreme judgments toward themselves, which is disruptive of appropriate performance. Reducing mental isolation provides more interaction with others and leads to acquiring various leaving experiences for individuals [37].
Individuals with high self-compassion, high self-acceptance, and low self-criticism, feel valued. Additionally, in experiencing unpleasant events that involve social evaluation and comparison, they know that all humans may make mistakes and commit wrong things, so they experience less negative feelings (human common things factors). They accept their mistakes and try to compensate instead of drowning in negative emotions and blame himself/herself, feeling lonely and being alone, so they never lose their self-esteem. Generally speaking, individuals with self-compassion are more optimistic and, therefore, can better cope with their negative emotions (as one of the positive factors). Also, training and practices which have been performed to increase self-compassion can be effective in improving different forms of disorders [38].
Conclusion
In this study, the effectiveness of positive psychology and self-compassion training on cognitive flexibility and cognitive failure were examined in girls with primary dysmenorrhea. Although self-compassion and positive psychology training did not affect cognitive flexibility, they were effective in improving girl’s cognitive failure. This study had some limitations. Some students did not cooperate in homework assignments and did not take non-pharmacological methods seriously. Also, the results cannot be generalized.
In addition, due to time limitation and lack of access to students, the follow-up stage was not performed. To achieve conclusive results, it is recommended to conduct future research in other populations with dysmenorrhea and investigate the effect in the follow-up stage.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of the Islamic Azad University of Rasht branch on September 24, 2018 (IR.IAURASHT.REC.1397.006). All the study procedures were in compliance with the ethical guidelines of the Declaration of Helsinki, 2013.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
Coceptualization, methodology: All authors; Investigation: Karameh Saghebi Saeedi; Writing-original draft: Karameh Saghebi Saeedi; Writing- review & editing: Abbas Abolghsemi, Karameh Saghebi Saeedi; Funding acquisition, resources: Karameh Saghebi Saeedi; Supervision: Abbas Abolghasemi, Bahman Akbari.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors appreciate the education officials of district one, school principals, and students who sincerely contribute to perform this study.
References
Aksu H, Özsoy S. Primary dysmenorrhea and herbals. J Health Commun. 2016; 1(23):1-3. [DOI:10.4172/2472-1654.100023]
Abaraogu UO, Tabansi-Ochuogu CS. As acupressure decreases pain, acupuncture may improve some aspects of quality of life for women with primary dysmenorrhea: A systematic review with meta-analysis. J Acupunct Meridian Stud. 2015; 8(5):220-8. [DOI:10.1016/j.jams.2015.06.010] [PMID]
Speroff L, Glass RH, Kase NG. Clinical gynecologic endocrinology and infertility. 6th ed. Baltimore: Lippincott, Williams & Wilkins; 1999.
Gilasi G, Suki Z, Kohzadi SH, Khasi B. [Investigate the prevalence of dysmenorrhea and some related factors in female students in Kashan University of Medical Sciences (Persian)]. Zanko J Med Sci. 2015: 28-34.
Ibrahim NK, AlGhamdi MS, Al-Shaibani AN, Ali-AlAmri F, Abdulrahman-Alharbi H, Al-Jadani AK, et al. Dysmenorrhea among female medical students in King Abdulaziz University: Prevalence, predictors and outcome. Pak J Med Sci. 2015; 31(6):1312-7. [DOI:10.12669/pjms.316.8752] [PMID] [PMCID]
Al-Kindi R, Al-Bulushi A. Prevalence and impact of dysmenorrhea among Omani. Sultan Qaboos Uni Medl J. 2011; 11(4):485-91.
Unsal A, Ayranci U, Tozun M, Arsalan G, Calik E. Prevalence dysmenorrhea and its effect on quality of life among a group of female university students. Upsala J Med Sci. 2010; 115:138-45. [DOI:10.3109/03009730903457218] [PMID] [PMCID]
Charu S, Amita R, Sujoy R, Thomas JA. Menstrual characteristics’ and ‘prevalence and effects of dysmenorrhea on quality of life of medical students. Int J Collab Res Intern Med Pubic Health. 2012; 4(4):276-94.
Zahradnik H-P, Hanjalic-Beck A, Groth K. Nonsteroidal anti-inflammatory drugs and hormonal contraceptives for pain relief from dysmenorrhea: A review. Contracept. 2010; 81(3):185-96. [DOI:10.1016/j.contraception.2009.09.014] [PMID]
Chen HY, Lin YH, Su IH, Chen YC, Yang SH, Chen JL. Investigation on Chinese herbal medicine for primary dysmenorrhea: Implication from a nationwide prescription database in Taiwan. Complement Ther Med. 2014; 22(1):116-25. [DOI:10.1016/j.ctim.2013.11.012] [PMID]
Sanaat Negar S, Rostami R. [Traumatic brain damage and effectiveness of cognitive rehabilitation in the improvement of attention, memory and exclusive function of affected patients (Persian)]. GenPsych. 2014; 3(7):63-80.
Gabrys RL, Tabri N, Anisman H, Matheson K. Cognitive control and flexibility in the context of stress and depressive symptoms: The cognitive control and flexibility questionnaire. Front Psychol. 2018; 9:2219. [DOI:10.3389/fpsyg.2018.02219] [PMID] [PMCID]
Unsworth N, Brewer GA, Spillers GJ. Variation in cognitive failures: An individual differences investigation of everyday attention and memory failures. J Mem Lang. 2012; 67:1-16. [DOI:10.1016/j.jml.2011.12.005]
Tirre WC. Dimensionality and determinants of self-reported cognitive failures. Int J Psychol Res. 2018; 11(1):9-18. [DOI:10.21500/20112084.3213]
Carbonella JY, Timpano KR. Examining the link between hoarding symptoms and cognitive flexibility deficits. Behav Ther. 2016; 47(2):262-73. [DOI:10.1016/j.beth.2015.11.003] [PMID]
Ionescu T. When is a cognitive system flexible? The variability-stability-flexibility pattern on the way to novel solutions. AVANT. 2017; 8:252-64. [DOI:10.26913/80s02017.0111.0023]
Meiran N, Diamond GM, Toder D, Nemets B. Cognitive rigidity in unipolar depression and obsessive compulsive disorder: Examination of task switching, stroop, working memory updating and post-conflict adaptation. Psychiatry Res. 2011; 185:149-56. [DOI:10.1016/j.psychres.2010.04.044] [PMID]
Fazeli M, Ehteshamzadeh P, Hashemi Sheikh Bahani E. [The effectiveness of cognitive behavior therapy on cognitive flexibility of depressed people (Persian)]. Thought Behav Clin Psychol. 2014; 9(34):27-36.
Soltani E, Shareh H, Bahrainian A, Farmani A. [The mediating role of cognitive flexibility in correlation of coping styles and resilience with depression (Persian)]. Pejouhandeh. 2013; 18(2):88-96.
Stone WS, Iguchi L. Stress and mental flexibility in autism spectrum disorders. N Am J Med Sci. 2013; 3(6):145-53.
Cheragh sahar Z, Atashpoor H. [The effectiveness positive cognitive-behavioural training in children mother’s cognitive flexibility affected by defeat hyperactivity disorder. Third national meeting of developing and promoting (Persian)]. Tehran, Association for the development and promotion of science and technology. 2015.
Abdi R, Chalabianloo G, Jabari G. [Effect of mindfulness practices on executive functions of elementary school students (Persian)]. Plant Cell Physiol. 2016; 4(1):9-16
Zare H. [Effectiveness of acceptance and commitment therapy (ACT) on improving the flexibility and cognitive fusion (Persian)]. Soc Cogn. 2017: 6(1):125-34.
Abbasi M, Pirani Z, Dargahi Sh, Bonyadi F. [Role of procrastination and motivational self-regulation in predicting students’ academic engagement (Persian)]. Iran J Med Educ. 2015; 15:160-9.
Abolghasemi A. [Psychological test. (Persian)]. Ardabil: Baghe Rezvan Press; 2005
Carrigan N, Barkus E. A systematic review of cognitive failures in daily life: Healthy populations. Neurosci Biobehav Rev. 2016; 63:29-42. [DOI:10.1016/j.neubiorev.2016.01.010] [PMID]
Abolghasemi A, Kiyamarei A. [The relationship between metacognition and cognitive failures in the elderly (Persian)]. Adv Cogn Sci. 2009; 11(1):8-15.
Mir Nasab MM, Mansour M, Afrouz GHA, Ghobari Bonab B, Behpaghouh A. [Impact of behavior therapy and cognitive-behavior therapy on amelioration of ADHD symptoms (Persian)]. J Except Child. 2008; 8(1):70-84.
Gilbert P. Compassion focused therapy: Special issue. Int J Cog Ther. 2010; 3(2):95-201. [DOI:10.1521/ijct.2010.3.2.95]
Taghavi Z. [Effectiveness of cognitive-behavioural therapy on reducing symptoms and increasing children self-control who have deficit hyperactivity disorder (Persian)]. [MA Thesis]. Tehran: Allame Tabatabaei University; 2010.
Teper R, Inzlicht M. Meditation, mindfulness and executive control. Soc Cog Affect Neurosci. 2013; 8(1):85-92. [DOI:10.1093/scan/nss045] [PMID] [PMCID]
Braehler C, Gumley A, Harper J, et al. Exploring change processes in compassion focused therapy in psychosis: Results of a feasibility randomized controlled trial. Br J Clin Psych 2013; 52(2):199-214. [DOI:10.1111/bjc.12009] [PMID]
Smeets E, Neff KD, Alberts H, Peters M. Meeting suffering with kindness: Effects of a brief self-compassion intervention for female college students. J Clin Psychol. 2014; 70(9):794-807. [DOI:10.1002/jclp.22076] [PMID]
Asadi S, Abolghasemi, A, Basharpoor S. [The effectiveness of mindfulness- based cognitive therapy on cognitive failure and emotional processing in anxious nurses (Persian)]. Iran J Neonatol. 2016; 29(102):55-65. [DOI:10.29252/ijn.29.102.55]
Noguchi K. Mindfulness as an end-state: Construction of a trait measure of mindfulness. Pers Individ Dif. 2017; 106:298-307. [DOI:10.1016/j.paid.2016.10.047]
Abbariky A, Yazdanbakhsh K, Momeni k. [The effectiveness of computer-based cognitive rehabilitation on reducing cognitive failure in students with learning disability (Persian)]. Q Psychol Except Individ. 2017; 7(26):127-57.
Narimani M, Einy S, Tagavy R. [Explaining students’ academic burnout based on self-compassion and sense of coherence (Persian)]. Jefferson Cent Ment Health. 2018; 5(1):36-47.
GhadamPoor E, Mansouri L. [The effectiveness of compassion-focused therapy on increasing optimism and self-sufficiency in female students with anxiety disorders (Persian)]. Gen Psychol Stud. 2018; 14(1):59-74.
Mohamed H, Neaem S. The effect of dysmenorrhea on quality of life of technical secondary schools girls. Med J Cairo Uni. 2013; 81(2):83-9.
Kannan P, Claydon LS. Some physiotherapy treatments may relieve menstrual pain in women with primary dysmenorrhea: A systematic review. J Physiother. 2014; 60(1):13-21. [DOI:10.1016/j.jphys.2013.12.003] [PMID]
She Y, Ma L, Zhu J, Qi C, Wang Y, Tang L, et al. Comparative study on skin temperature response to mensturationat acupuncture points in healthy volunteers and primary dysmenorrhea patients. J Tradit Chin Med Sci. 2017; 37(2):220-8. [DOI:10.1016/S0254-6272(17)30048-1]
Chen Chen X, Draucker Claire B, Carpente Janet S. What women say about their dysmenorrhea: A qualitative thematic analysis. BMC Womens Health. 2018; 18(47):1-17. [DOI:10.1186/s12905-018-0538-8] [PMID] [PMCID]
Ghomari Givi H, Sharei SJ, Mohammadipour Rik N, et al. [Evaluation of the effectiveness of relaxation and distraction techniques to reduce and Pain control in hospitalized children (Persian)]. Couns Psychother Cult. 2012; 3(10):101-15.
Seligman MEP, Ernst RM, Gillham J, Reivich K, Linkins, M. Positive education: Positive psychology and classroom interventions. Oxf Rev Educ. 2009; 35(3):293-311. [DOI:10.1080/03054980902934563]
Nick Manesh Z, Zandvokil M. [The effect of positive thinking training on quality of life, depression, stress and anxiety in delinquent juveniles (Persian)]. Posit Psychol Res. 2015; 1(2):53-64.
Hayes L, Ciarrochi J. The thriving adolescent: Using acceptance and commitment therapy and positive psychology to help young people manage emotions, achieve goals, and build positive relationships. Oakland. CA: Context Press; 2015.
Neff KD. Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self Identity. 2003; 2:85-102. [DOI:10.1080/15298860309032]
Yanel LM, Neff KD. Self-compassion, interpersonal conflict. Resolution, and well- being. Self Identity. 2013; 12:146-59. [DOI:10.1080/15298868.2011.649545]
Akin A, Akin U. Self-compassion as a predictor of social safeness in Turkish university students. Revista Latinoam Psicología. 2015; 47(1):43-9. [DOI:10.1016/S0120-0534(15)30005-4]
Sirois MF. A self-regulation resource model of self-compassion and health behavior intentions in emerging adults. Prev Med Rep. 2015; 2:218-22. [DOI:10.1016/j.pmedr.2015.03.006] [PMID] [PMCID]
Dunne S, Sheffield D, Chilcot J. Brief report: Self-compassion, physical health and the mediating role of health-promoting behaviours. J Health Psychol. 2018; 23(7):993-9. [DOI:10.1177/1359105316643377] [PMID]
Brown L, Bryant C, Brown, V, Bei B, Judd F. Self-compassion, attitudes to ageing and indicators of health and well-being being among midlife women. Aging & Mental Health. 2016; 20(10):1035-43. [DOI:10.1080/13607863.2015.1060946] [PMID]
Bluth K, Eisenlohr-Moul TA. Response to a mindful self-compassion intervention in teens: A within-person association of mindfulness, self-compassion, and emotional well-being outcomes. J Adolesc. 2017; 57:108-18. [DOI:10.1016/j.adolescence.2017.04.001] [PMID] [PMCID]
Siahpour T, Nikbakht M, Rahimi A, Rabiei MA. [Effect of eight weeks aerobic training and yoga on primary dysmenorrhea (Persian)]. Armaghane Danesh. 2013; 18(6):475-83.
Reyhani T, Jafarnezhad F, Hosseini B, Ajam M, Baghaei M. [Investigating the effect of fast walking on girl student’s dysmenorrhea and women infertility (Persian)]. Iran J Obstet, Gynaecol Infertil. 2013; 16(46):14-9.
Jamali F, Moazzami M, Bijan N. [The effect of eight weeks aerobic training on serum beta-endorphosis and perception of dysmenorrhea in inactive teenage girls (Persian)]. J Sabzevar Uni Med Sci 2014; 21(14):702-10.
Farshbaf Mani Sefat F, Abolghasemi A, Borhanmand O, Hajloo N. [Comparison of the effectiveness of cognitive-behavioral therapy and hypnotherapy therapy on pain self-efficacy and pain severity in girls with primary dysmenorrhea (Persian)]. Armaghane Danesh. 2017; 22(1):87-103.
Siahbazi SH, Hariri FZ, Montazeri A, Moghaddam Banaem L. [Translation and psychometric properties of the Iranian version of the Premenstrual Symptoms Screening Tool (PSST) (Persian)]. Payesh. 2011; 10(4):421-7.
Dennis JP, Vander Wal JS. The cognitive flexibility inventory: Instrument development and estimates of reliability and validity. Cognit Ther Res. 2010; 34:241-53. [DOI:10.1007/s10608-009-9276-4]
Wallace JC, Vodanovich SJ, Restino BM. Predicting cognitive failures from boredom proneness and daytime sleepiness scores: An investigation within military and undergraduate samples. Pers Individ Dif. 2003; 34:635-44. [DOI:10.1016/S0191-8869(02)00050-8]
Abolghasemi A. Investigating the relationship between metacognitive and religious beliefs with cognitive failures in older and older people. Ardabili: University of Mohaghegh Ardabili; 2007.
Rashid T. Positive psychotherapy: Exploring the best in people. In: Shane J. Lopez, editor. Positive Psychology: Pursuing Human Flourishing. Westport: Praeger; 2008.
Neff KD, Germer CK. A pilot study and randomized controlled trial of the mindful self-compassion program. J Clin Psychol. 2013; 69(1):28-44. [DOI:10.1002/jclp.21923] [PMID]
Type of Study: Research |
Subject:
Special
Received: 2020/05/23 | Accepted: 2020/05/23 | Published: 2020/05/23
Received: 2020/05/23 | Accepted: 2020/05/23 | Published: 2020/05/23
Send email to the article author
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
