Thu, Apr 25, 2024
Volume 3, Issue 2 (Spring 2017)
Caspian J Neurol Sci 2017, 3(2): 95-105 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Madjidzadeh R, Hakimjavadi M, Gholamali Lavasani M. The Reduction of Anxiety and Blood Sugar Level with Group Cognitive-Behavior Therapy in Men and Women with Type II Diabetes: An Experimental Study
. Caspian J Neurol Sci 2017; 3 (2) :95-105
URL: http://cjns.gums.ac.ir/article-1-180-en.html
URL: http://cjns.gums.ac.ir/article-1-180-en.html


1- University of Guilan, Rasht, Iran; Email: majidzadehroya@gmail.com
2- Associate Professor of Psychology, University of Guilan, Rasht, Iran
3- Associate Pofessor of Psychology, University of Tehran, Tehran, Iran
2- Associate Professor of Psychology, University of Guilan, Rasht, Iran
3- Associate Pofessor of Psychology, University of Tehran, Tehran, Iran
Full-Text [PDF 885 kb]
(1709 Downloads)
| Abstract (HTML) (3546 Views)
Full-Text: (1401 Views)
ABSTRACT
Background: Although psychological distress can interfere with diabetes care, the effectiveness of Group Cognitive-Behavior Therapy in improving diabetes outcomes is unknown.
Objectives: The purpose of this study was to reduce anxiety symptoms and improve glycemic control in diabetic patients. The samples were 24 diabetic patients (12 in experimental group and 12 in control group) aging from 40 to 60 years.
Materials and Methods: The anxiety symptoms and glycemic control were assessed prior to and following Group Cognitive-Behavior Therapy (CBT) using self-report instruments and through measuring glycosylated hemoglobin and fasting blood sugar (FBS). SPSS software version 16 was also used for statistical analysis of the study.
Results: The results, analyzed by the analysis of covariance, indicated that after group-therapy, there were no significant differences between the two groups in as far as the means of FBS concentration. Moreover, a significant decrease was seen in hemoglobin A1c (HbA1c) concentration after group-therapy in the experimental group. As far as anxiety, no significant difference was observed between the two groups following the therapy; however, after group therapy, the anxiety of the women in the experimental group underwent a significant decrease. In addition, a reduction in anxiety symptoms was observed post group-therapy, and the reoccurred significant changes in the glycemic control.
Conclusion: The findings of this pilot study suggest that group-therapy is a feasible intervention for patients with diabetes and anxiety symptoms. However, further research is needed if a development is to be had regarding the interventions that improve glycemic control.
Keywords: Anxiety; Psychotherapy; Diabetes Mellitus
Introduction
Socio-psychological conditions can elicit immunological-physiological responses, lowering the resistance to diseases. Hyper-stimulation may cause excessive autonomic and cortical arousal leading to cognitive and motor performance.
Repeated or sustained arousal can entail physiological changes as well as changes in behavior, enhancing the subject’s general susceptibility to illnesses [1].
Diabetes mellitus belongs to the category of psycho-physiological disorders that indicate the existence of a physical illness closely connected to cognitive structures in humans in a way that their interactions have been noted by researchers in medical and psychological area [2]. On the other hand, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), the diagnostic criteria for psycho-cognitive factors affecting medical conditions include: the existence of a medical illness, and also the psychological factors affecting the procedure of illness and prevent its treatment.
Concerning diabetes, constantly reported is the presence of mental pressure and anxiety factors such as stress and depression [3-5].
Diabetes can be associated with some major psychological and physical problems such as cardiac disorder, chronic kidney disease, blindness, autonomic nervous system damage, anxiety, depression, functional cognitive disorders, delirium and delusion. Although psychological stressful events may slightly influence the onset of diabetes in patients who are prone to it, they may develop the clinical symptoms of diabetes in patients through increasing the demand for the secretion of insulin from those B cells already depleted [6].
Diabetes has a negative impact on the function of central and peripheral nervous systems. A diabetic patient, for instance, is very sensitive over reacting to stress. Stressful events may worsen the symptoms and the severity of diabetes through increasing the demand for insulin secretion by B cells.
Among the anxiety disorders observed in patients, Generalized Anxiety Disorder (GAD) has a higher prevalence (nearly 40 percent) causing more impairment in the patient [7]. Given the estimated prevalence of anxiety in diabetic patients, more measures should be taken so as to prevent anxiety disorders. Whereas anxiety has a substantial negative impact on the quality of life in diabetic patients and severely impacts family life and daily routines, social and cognitive assessment should also be taken into consideration as a part of special care for diabetics. As was mentioned earlier, diabetic patients get upset very easily and experience rapid changes in behavior. Studies have shown that anxiety disorders reduce the quality of life in patients with Diabetes Mellitus [8]. Therefore, both social and psychological aspects should be assessed as the main basis for the treatment of diabetes.
The purpose of psychophysical disorder therapy is to eradicate psycho-physiological factors and to prevent them from reoccurring. Basic psycho-cognitive factors have to be focused on alongside physical factors, hence the fact that medical treatment is not the only choice in the treatment of diabetics. A diabetic patient should be motivated to go through treatment interventions and make the changes in their life style. The need for effective psychological interventions in diabetes has long been recognized [9] with the main focus on reducing the psychological and behavioral impact of anxiety on metabolic control.
According to studies, anxiety and depression result in high levels of glycosylated hemoglobin in blood [10,11]. There exist various cases where following psychological interventions, high levels of hemoglobin “A1c” were observed.
Recent approaches to the treatment of psychological disorders include medical treatment and also psychological, physiological and cognitive-behavioral approaches. Identification of the appropriate approach, however, is not facile as the disorders depend on a set of genetic environmental, biochemical and physiological factors. A recent study carried out in Africa pointed out that psychological and mental problems such as anxiety are closely related to physical diseases such as diabetes which can be managed by psychological interventions [12].
Due to the social significance of human life, the individual’s behavior and interaction with others has an effective impact on their physical and mental health. Psychotherapy is a reciprocal, psycho-physical interaction and the friendliness and sympathy of the psychotherapist may result in physiological changes in the patients. On the other hand, the patients undergoing therapy should make meaningful interactions with others and be able to make logical reciprocal relations to overcome the psycho-physical factors of anxiety.
Therefore, the cognitive-behavioral approach should be applied in the form of group therapy. The main purposes in group therapy sessions with cognitive-behavioral approach are to reduce anxiety factors, to provide anxiety prevention strategies, and to improve the patients’ self-efficacy.
In a certain study carried out in 2015, the group therapy with the cognitive-behavioral approach had an effective but short term impact on the anxiety reduction and the improvement of the quality of life in diabetic patients [13].
In the cognitive-behavioral group therapy sessions, usually the following steps should be followed. First, an introduction is provided and the regulations are elucidated. Then, the impact of the individual’s thought on his or her behavior is evaluated. The frequently asked questions in therapy are as follows: “what is anxiety?” What are the thoughts of anxious people?”, “What are the strategies to induce positive thoughts?”, “How can negative thoughts be expressed?”, “How should one evaluate the impact of activities on one’s behavior using suitable timing and setting specific goals?” The next steps are programming such soothing activities as muscle relaxation, and evaluating the effect of interaction on patient behavior through creating support networks, allowing patients to communicate with new people and gain self-improvement skills. The sessions are finally evaluated and the feedbacks elicited [14].
The present study was carried out on patients suffering from diabetes mellitus (type II). Because of gradual growth of the disease, and discussed impact of the disease the present study aimed to evaluate the impact of psychological interventions (cognitive-behavioral approach) on type II diabetic patients regarding the levels of A1C hemoglobin, the blood glucose and anxiety.
Material and Methods
In this study, diabetic patients were referred to a clinical diagnostic lab located in the city of Rezvanshahr, northern Iran. Sampling was conducted in three consecutive months, during which period 100 diabetics were selected according to the required variables of the study and diabetic conditions stipulated by American Diabetes Association (ADA). In order to examine the research questions with regard to the type of the research design which was experimental, the
researcher considered a sample size of 24 patients (α<0.05), and divided them into two groups of experimental and control (figure 1).
The minimum sample size for measuring the effectiveness of the study intervention was calculated by using the Cohen’s table [15].
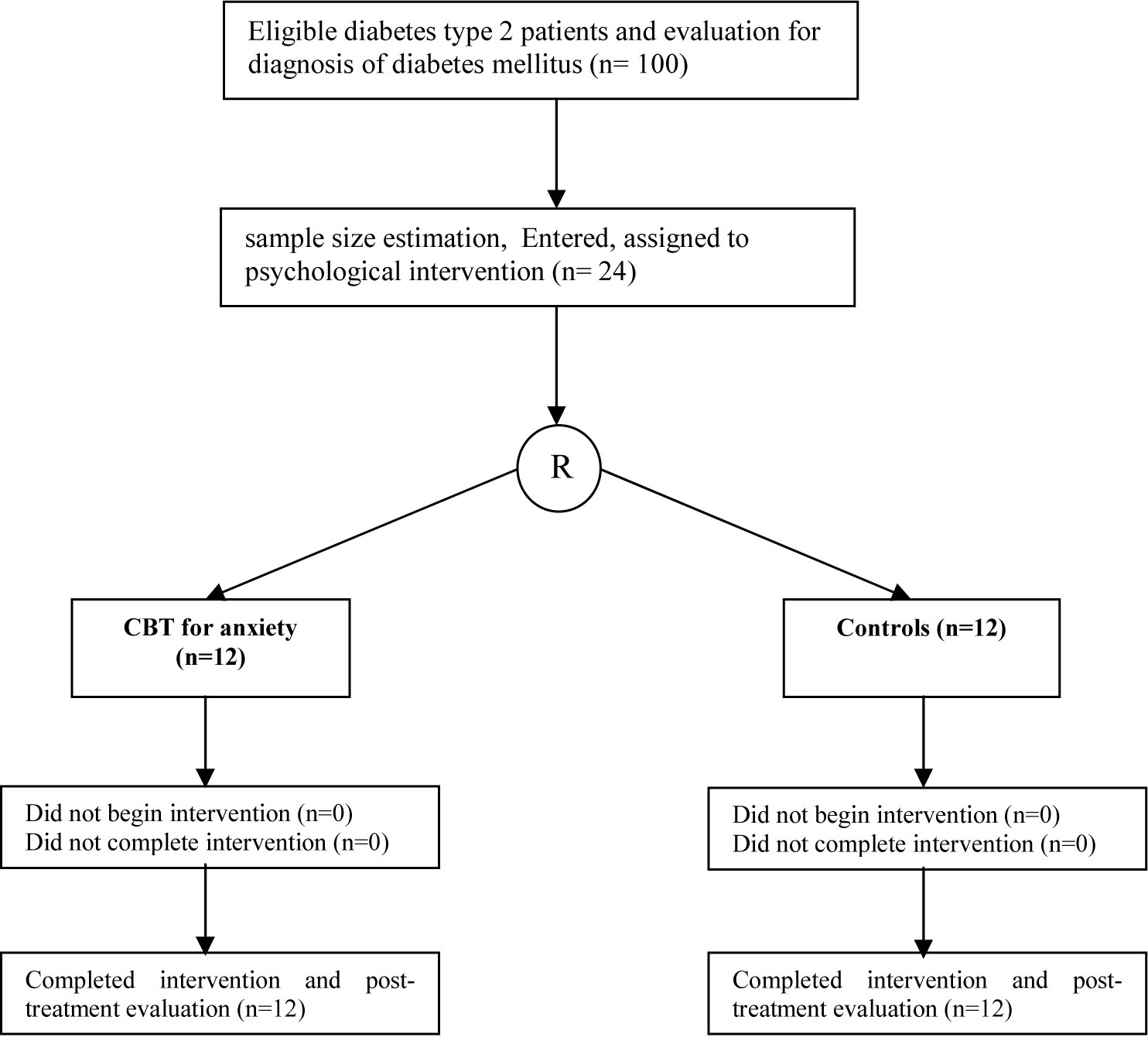
Figure 1. Study participation data. CBT: cognitive behavior therapy, R: randomization
The results showed that with a confidence interval of 0.05, an effect size of 0.80, and a power of 0.90, twelve participants were needed for each group. Patients who met the inclusion criteria and gave informed consent underwent a 1-week period of glucometer training and baseline assessment, after which they were randomly assigned to study groups. There were equal numbers of male and female in each group with the age range of 40-60.If any change occurred in all the medication used by the patient which can change the serum level of glucose he/she excluded from study.
Measures
Zung Self-Rating Anxiety Scale (SAS): This questionnaire has 20 multiple choice questions and is prepared based on the physical symptoms of emotional distress. SAS has 5 diagnostic criteria for emotional signs and 15 for physical symptoms. When using this scale, the patients are asked to respond to each of the 20 questions based on their true experience during the week before. In SAS, people who have less anxiety acquire lower scores and vice versa. The SAS possess validity because of its construction on the basis of DSM-II diagnostic criteria (i.e., both somatic and cognitive/emotional symptoms, such as worrying, feeling hopeless, and sleeplessness, lack of enjoyment of life, muscle tremors, stomach churning, sweating and increased frequency of urination). Reliability data for the SAS is satisfactory at 0.71 [16], and a coefficient alpha of 0.85 has been reported [17], indicating acceptable levels of internal consistency.
Generalized Anxiety Disorder 7-item (GAD-7) scale: This questionnaire has seven multiple-choice questions to be answered based on the patients’ true experience during the foregoing two weeks. In scale GAD-7, those with more anxiety receive higher scores. According to previous studies [18] the internal consistency of the GAD-7 was excellent (Cronbach α = 0.92). Test-retest reliability was also good (intraclass correlation = 0.83). Comparison of scores derived from the self-report scales with those derived from the MHP-administered versions of the same scales yielded similar results (intraclass correlation = 0.83), indicating good procedural validity [18].
Fasting Blood Glucose Monitoring: Blood glucose levels were determined by an enzymatic glucose oxidase assay. In this assay, the generated peroxide is converted into Quinone imine indicator in the presence of Amino Phenazone 4 and phenol. The color intensity directly correlated with the concentration of blood glucose. It should be mentioned that in this method, serum or plasma can also be used. Measuring was carried out using an auto analyzer system and at a wavelength of 495 nm. The time for measuring FBS glucose was at 9 AM and the time of the presence of the patients at 7 AM for blood-letting.
Glycosylated hemoglobin: The hemoglobin A1c (HbA1c) or glycosylated hemoglobin levels were determined by an ion exchange chromatography method. Ion exchange columns were equilibrated by phosphate buffer 72 mmol/l. The hemolysate sample was passed through a column and the absorbance of the eluted fraction was monitored in 415 nm using a spectrophotometer. The level of HbA1c was reported in percentage.
After determining the sample groups (experimental and control groups), the study instruments (Zung Anxiety Scale and a questionnaire 7) were distributed. Next, fasting blood glucose tests and hemoglobin A1c tests were carried out on both groups. The groups were prepared to participate in group therapy sessions in the presence of a psychotherapist. After a three-month interval from the end of intervention, all the above tests and processes were carried out again for both groups. The psychological intervention place was in the auditorium of Payame Noor University in Rezvanshahr city and its time was between 16:00 to 18:00 in the afternoon. All blood samples were analyzed in a laboratory with a similar kit, and all psychological interventions were performed by a therapist. The research data were processed using SPSS version 16.0, through univariate and multivariate analysis of variance.
Group therapy sessions
Session I: In the first session, the group members met and provided a brief explanation of the unphysical conditions and medical history. After that, the leader explained the purpose of the meeting starting by an introduction on CBT and diabetes, and explaining the regulations of group therapy.
Session II: The second session started by focusing on “What is diabetes?” The diabetes treatment triangle (diet, exercise, medication) was also introduced to the patients and the possible strategies to control and manage the disease were discussed.
Sessions III and IV: The main issue in these sessions was "How thought affects our behavior?" The patients were asked to ace their wrong beliefs and try to correct it. They were encouraged to accept their negative thoughts since avoiding them might result in anxiety.
So as to create a positive attitude to deal with negative thoughts, imagery techniques, mental judgment and mind review/recall were practiced with group members. Intellectual traps such as unrealistic expectations, unreason able responsibilities and the comparison of self against others were investigated.
Sessions V and VI: "How activities affect our moods" was the main issue in these sessions. Pleasant activities, proper timing and setting specific purposes were proposed.
Session VII: The topic of "How do interpersonal relationships affect our moods?" was discussed in this session. Participating in social support networks, meeting new people and self-improvement skills were also examined as ways of reducing anxiety.
Session VIII: After the revision and evaluation of the previous steps, the patients’ feedbacks on each topic were followed. These sessions were based on previous studies [4,19].
Ethics
The study was approved by the Ethics Committee (postgraduate council for department of psychology) University of Guilan (23404-18). Written informed consent form was signed by all the participants.
Results
The average age and the standard deviation of the experimental group and the control group were 46.6 and 6.28 SD, respectively. The history of diabetes mellitus (type II) in the selected population was under 10 years. Since the experimental design of this study was based on repeated measurements, hemoglobin A1c and fasting plasma glucose concentration was measured before and after group therapy. Analysis of covariance was employed in order to examine the main effects of gender and group, and their interactional effect on dependent variables (table 1).
According to table 1, the results showed no significant difference in FBS variable at p<0.05. The interactive effect of Group by gender was not also significant for gender variable. The results show significant differences in glycosylated hemoglobin variable between the two groups at p<0.05. Considering the means shows that the experimental group in the HbA1c has obtained averages in comparison with the control group (7.71 versus 8.06). To examine the effect of group and gender on the level of anxiety in participants, the analysis of covariance was used. The results indicate no significant difference between the groups at p<0.05. The difference between genders was not significant either. The statistical features analysis of general anxiety description (GAD) dependents (after group therapy) indicates that the mean of squares in female experimental group is less than the male experimental group whereas the mean of squares in female control group is higher than the male control group (table 2).
Table 3 shows the results of GAD covariance in examining the possible effect of group and gender on the level of anxiety.
The results indicate that the main effect of gender and group was not significant; however, the interactive effect of group by gender was significant, meaning that probably the intervention has different impacts on males and females. To examine this statement, the simple effect of group and gender was calculated (table 4).
Background: Although psychological distress can interfere with diabetes care, the effectiveness of Group Cognitive-Behavior Therapy in improving diabetes outcomes is unknown.
Objectives: The purpose of this study was to reduce anxiety symptoms and improve glycemic control in diabetic patients. The samples were 24 diabetic patients (12 in experimental group and 12 in control group) aging from 40 to 60 years.
Materials and Methods: The anxiety symptoms and glycemic control were assessed prior to and following Group Cognitive-Behavior Therapy (CBT) using self-report instruments and through measuring glycosylated hemoglobin and fasting blood sugar (FBS). SPSS software version 16 was also used for statistical analysis of the study.
Results: The results, analyzed by the analysis of covariance, indicated that after group-therapy, there were no significant differences between the two groups in as far as the means of FBS concentration. Moreover, a significant decrease was seen in hemoglobin A1c (HbA1c) concentration after group-therapy in the experimental group. As far as anxiety, no significant difference was observed between the two groups following the therapy; however, after group therapy, the anxiety of the women in the experimental group underwent a significant decrease. In addition, a reduction in anxiety symptoms was observed post group-therapy, and the reoccurred significant changes in the glycemic control.
Conclusion: The findings of this pilot study suggest that group-therapy is a feasible intervention for patients with diabetes and anxiety symptoms. However, further research is needed if a development is to be had regarding the interventions that improve glycemic control.
Keywords: Anxiety; Psychotherapy; Diabetes Mellitus
Introduction
Socio-psychological conditions can elicit immunological-physiological responses, lowering the resistance to diseases. Hyper-stimulation may cause excessive autonomic and cortical arousal leading to cognitive and motor performance.
Repeated or sustained arousal can entail physiological changes as well as changes in behavior, enhancing the subject’s general susceptibility to illnesses [1].
Diabetes mellitus belongs to the category of psycho-physiological disorders that indicate the existence of a physical illness closely connected to cognitive structures in humans in a way that their interactions have been noted by researchers in medical and psychological area [2]. On the other hand, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), the diagnostic criteria for psycho-cognitive factors affecting medical conditions include: the existence of a medical illness, and also the psychological factors affecting the procedure of illness and prevent its treatment.
Concerning diabetes, constantly reported is the presence of mental pressure and anxiety factors such as stress and depression [3-5].
Diabetes can be associated with some major psychological and physical problems such as cardiac disorder, chronic kidney disease, blindness, autonomic nervous system damage, anxiety, depression, functional cognitive disorders, delirium and delusion. Although psychological stressful events may slightly influence the onset of diabetes in patients who are prone to it, they may develop the clinical symptoms of diabetes in patients through increasing the demand for the secretion of insulin from those B cells already depleted [6].
Diabetes has a negative impact on the function of central and peripheral nervous systems. A diabetic patient, for instance, is very sensitive over reacting to stress. Stressful events may worsen the symptoms and the severity of diabetes through increasing the demand for insulin secretion by B cells.
Among the anxiety disorders observed in patients, Generalized Anxiety Disorder (GAD) has a higher prevalence (nearly 40 percent) causing more impairment in the patient [7]. Given the estimated prevalence of anxiety in diabetic patients, more measures should be taken so as to prevent anxiety disorders. Whereas anxiety has a substantial negative impact on the quality of life in diabetic patients and severely impacts family life and daily routines, social and cognitive assessment should also be taken into consideration as a part of special care for diabetics. As was mentioned earlier, diabetic patients get upset very easily and experience rapid changes in behavior. Studies have shown that anxiety disorders reduce the quality of life in patients with Diabetes Mellitus [8]. Therefore, both social and psychological aspects should be assessed as the main basis for the treatment of diabetes.
The purpose of psychophysical disorder therapy is to eradicate psycho-physiological factors and to prevent them from reoccurring. Basic psycho-cognitive factors have to be focused on alongside physical factors, hence the fact that medical treatment is not the only choice in the treatment of diabetics. A diabetic patient should be motivated to go through treatment interventions and make the changes in their life style. The need for effective psychological interventions in diabetes has long been recognized [9] with the main focus on reducing the psychological and behavioral impact of anxiety on metabolic control.
According to studies, anxiety and depression result in high levels of glycosylated hemoglobin in blood [10,11]. There exist various cases where following psychological interventions, high levels of hemoglobin “A1c” were observed.
Recent approaches to the treatment of psychological disorders include medical treatment and also psychological, physiological and cognitive-behavioral approaches. Identification of the appropriate approach, however, is not facile as the disorders depend on a set of genetic environmental, biochemical and physiological factors. A recent study carried out in Africa pointed out that psychological and mental problems such as anxiety are closely related to physical diseases such as diabetes which can be managed by psychological interventions [12].
Due to the social significance of human life, the individual’s behavior and interaction with others has an effective impact on their physical and mental health. Psychotherapy is a reciprocal, psycho-physical interaction and the friendliness and sympathy of the psychotherapist may result in physiological changes in the patients. On the other hand, the patients undergoing therapy should make meaningful interactions with others and be able to make logical reciprocal relations to overcome the psycho-physical factors of anxiety.
Therefore, the cognitive-behavioral approach should be applied in the form of group therapy. The main purposes in group therapy sessions with cognitive-behavioral approach are to reduce anxiety factors, to provide anxiety prevention strategies, and to improve the patients’ self-efficacy.
In a certain study carried out in 2015, the group therapy with the cognitive-behavioral approach had an effective but short term impact on the anxiety reduction and the improvement of the quality of life in diabetic patients [13].
In the cognitive-behavioral group therapy sessions, usually the following steps should be followed. First, an introduction is provided and the regulations are elucidated. Then, the impact of the individual’s thought on his or her behavior is evaluated. The frequently asked questions in therapy are as follows: “what is anxiety?” What are the thoughts of anxious people?”, “What are the strategies to induce positive thoughts?”, “How can negative thoughts be expressed?”, “How should one evaluate the impact of activities on one’s behavior using suitable timing and setting specific goals?” The next steps are programming such soothing activities as muscle relaxation, and evaluating the effect of interaction on patient behavior through creating support networks, allowing patients to communicate with new people and gain self-improvement skills. The sessions are finally evaluated and the feedbacks elicited [14].
The present study was carried out on patients suffering from diabetes mellitus (type II). Because of gradual growth of the disease, and discussed impact of the disease the present study aimed to evaluate the impact of psychological interventions (cognitive-behavioral approach) on type II diabetic patients regarding the levels of A1C hemoglobin, the blood glucose and anxiety.
Material and Methods
In this study, diabetic patients were referred to a clinical diagnostic lab located in the city of Rezvanshahr, northern Iran. Sampling was conducted in three consecutive months, during which period 100 diabetics were selected according to the required variables of the study and diabetic conditions stipulated by American Diabetes Association (ADA). In order to examine the research questions with regard to the type of the research design which was experimental, the
researcher considered a sample size of 24 patients (α<0.05), and divided them into two groups of experimental and control (figure 1).
The minimum sample size for measuring the effectiveness of the study intervention was calculated by using the Cohen’s table [15].
Figure 1. Study participation data. CBT: cognitive behavior therapy, R: randomization
The results showed that with a confidence interval of 0.05, an effect size of 0.80, and a power of 0.90, twelve participants were needed for each group. Patients who met the inclusion criteria and gave informed consent underwent a 1-week period of glucometer training and baseline assessment, after which they were randomly assigned to study groups. There were equal numbers of male and female in each group with the age range of 40-60.If any change occurred in all the medication used by the patient which can change the serum level of glucose he/she excluded from study.
Measures
Zung Self-Rating Anxiety Scale (SAS): This questionnaire has 20 multiple choice questions and is prepared based on the physical symptoms of emotional distress. SAS has 5 diagnostic criteria for emotional signs and 15 for physical symptoms. When using this scale, the patients are asked to respond to each of the 20 questions based on their true experience during the week before. In SAS, people who have less anxiety acquire lower scores and vice versa. The SAS possess validity because of its construction on the basis of DSM-II diagnostic criteria (i.e., both somatic and cognitive/emotional symptoms, such as worrying, feeling hopeless, and sleeplessness, lack of enjoyment of life, muscle tremors, stomach churning, sweating and increased frequency of urination). Reliability data for the SAS is satisfactory at 0.71 [16], and a coefficient alpha of 0.85 has been reported [17], indicating acceptable levels of internal consistency.
Generalized Anxiety Disorder 7-item (GAD-7) scale: This questionnaire has seven multiple-choice questions to be answered based on the patients’ true experience during the foregoing two weeks. In scale GAD-7, those with more anxiety receive higher scores. According to previous studies [18] the internal consistency of the GAD-7 was excellent (Cronbach α = 0.92). Test-retest reliability was also good (intraclass correlation = 0.83). Comparison of scores derived from the self-report scales with those derived from the MHP-administered versions of the same scales yielded similar results (intraclass correlation = 0.83), indicating good procedural validity [18].
Fasting Blood Glucose Monitoring: Blood glucose levels were determined by an enzymatic glucose oxidase assay. In this assay, the generated peroxide is converted into Quinone imine indicator in the presence of Amino Phenazone 4 and phenol. The color intensity directly correlated with the concentration of blood glucose. It should be mentioned that in this method, serum or plasma can also be used. Measuring was carried out using an auto analyzer system and at a wavelength of 495 nm. The time for measuring FBS glucose was at 9 AM and the time of the presence of the patients at 7 AM for blood-letting.
Glycosylated hemoglobin: The hemoglobin A1c (HbA1c) or glycosylated hemoglobin levels were determined by an ion exchange chromatography method. Ion exchange columns were equilibrated by phosphate buffer 72 mmol/l. The hemolysate sample was passed through a column and the absorbance of the eluted fraction was monitored in 415 nm using a spectrophotometer. The level of HbA1c was reported in percentage.
After determining the sample groups (experimental and control groups), the study instruments (Zung Anxiety Scale and a questionnaire 7) were distributed. Next, fasting blood glucose tests and hemoglobin A1c tests were carried out on both groups. The groups were prepared to participate in group therapy sessions in the presence of a psychotherapist. After a three-month interval from the end of intervention, all the above tests and processes were carried out again for both groups. The psychological intervention place was in the auditorium of Payame Noor University in Rezvanshahr city and its time was between 16:00 to 18:00 in the afternoon. All blood samples were analyzed in a laboratory with a similar kit, and all psychological interventions were performed by a therapist. The research data were processed using SPSS version 16.0, through univariate and multivariate analysis of variance.
Group therapy sessions
Session I: In the first session, the group members met and provided a brief explanation of the unphysical conditions and medical history. After that, the leader explained the purpose of the meeting starting by an introduction on CBT and diabetes, and explaining the regulations of group therapy.
Session II: The second session started by focusing on “What is diabetes?” The diabetes treatment triangle (diet, exercise, medication) was also introduced to the patients and the possible strategies to control and manage the disease were discussed.
Sessions III and IV: The main issue in these sessions was "How thought affects our behavior?" The patients were asked to ace their wrong beliefs and try to correct it. They were encouraged to accept their negative thoughts since avoiding them might result in anxiety.
So as to create a positive attitude to deal with negative thoughts, imagery techniques, mental judgment and mind review/recall were practiced with group members. Intellectual traps such as unrealistic expectations, unreason able responsibilities and the comparison of self against others were investigated.
Sessions V and VI: "How activities affect our moods" was the main issue in these sessions. Pleasant activities, proper timing and setting specific purposes were proposed.
Session VII: The topic of "How do interpersonal relationships affect our moods?" was discussed in this session. Participating in social support networks, meeting new people and self-improvement skills were also examined as ways of reducing anxiety.
Session VIII: After the revision and evaluation of the previous steps, the patients’ feedbacks on each topic were followed. These sessions were based on previous studies [4,19].
Ethics
The study was approved by the Ethics Committee (postgraduate council for department of psychology) University of Guilan (23404-18). Written informed consent form was signed by all the participants.
Results
The average age and the standard deviation of the experimental group and the control group were 46.6 and 6.28 SD, respectively. The history of diabetes mellitus (type II) in the selected population was under 10 years. Since the experimental design of this study was based on repeated measurements, hemoglobin A1c and fasting plasma glucose concentration was measured before and after group therapy. Analysis of covariance was employed in order to examine the main effects of gender and group, and their interactional effect on dependent variables (table 1).
| Table 1. Tree analysis of covariance the results of FBS, HbA1c, SAS regarding control and experimental group using Group- CBT, and between males and females | ||||||
| Dependent variable | Sources of changes | df | MS | F | p-value | ή2 |
| FBS (Mg / dl) | Groups | 1 | 1981.53 | 2.67 | 0.118 | 0.343 |
| gender | 1 | 1463.98 | 1.97 | 0.176 | 0.267 | |
| Group × gender | 1 | 1837.36 | 2.48 | 0.132 | 0.322 | |
| Error | 19 | 739.67 | ||||
| HbA1c | Groups | 1 | 1.23 | 6.24 | 0.022 | 0.659 |
| Gender | 1 | 0.104 | 0.527 | 0.447 | 0.106 | |
| Group × gender | 1 | 0.836 | 4.22 | 0.054 | 0.496 | |
| Error | 19 | 0.198 | ||||
| SAS | Groups | 1 | 2.56 | 0.447 | 0.512 | 0.097 |
| Gender | 1 | 13.42 | 2.33 | 0.143 | 0.306 | |
| Group × gender | 1 | 9.11 | 1.58 | 0.223 | 0.224 | |
| Error | 19 | 5.41 | ||||
| FBS: fasting blood sugar, HbA1c: hemoglobin A1c, SAS: Self-Rating Anxiety Scale | ||||||
According to table 1, the results showed no significant difference in FBS variable at p<0.05. The interactive effect of Group by gender was not also significant for gender variable. The results show significant differences in glycosylated hemoglobin variable between the two groups at p<0.05. Considering the means shows that the experimental group in the HbA1c has obtained averages in comparison with the control group (7.71 versus 8.06). To examine the effect of group and gender on the level of anxiety in participants, the analysis of covariance was used. The results indicate no significant difference between the groups at p<0.05. The difference between genders was not significant either. The statistical features analysis of general anxiety description (GAD) dependents (after group therapy) indicates that the mean of squares in female experimental group is less than the male experimental group whereas the mean of squares in female control group is higher than the male control group (table 2).
| Table 2. The Statistical features of GAD dependent variables in experimental group of Group-CBT and control group and between males and females | ||||
| Groups | Gender | Mean | SD | number |
| Experimental | Female | 9.33 | 2.33 | 6 |
| Male | 10 | 3.09 | 6 | |
| Control | Female | 10.33 | 1.21 | 6 |
| Male | 8.83 | 1.72 | 6 | |
| Total | Female | 9.83 | 1.85 | 12 |
| male | 9.41 | 2.46 | 12 | |
Table 3 shows the results of GAD covariance in examining the possible effect of group and gender on the level of anxiety.
| Table 3. The results of GAD covariance analysis in experimental group of Group-CBT and control group and between males and females | |||||
| Sources of changes | df | MS | F | p-value | ή2 |
| Groups | 1 | 1.34 | 1.14 | 0.298 | 0.174 |
| Gender | 1 | 0.538 | 0.46 | 0.506 | 0.099 |
| Group×gender | 1 | 6.03 | 5.15 | 0.036 | 0.578 |
| Error | 19 | 1.17 | |||
| Table 4. Simple effects of gender for groups (MANOVA) of Group- CBT and controls | ||||
| Source of changes | df | MS | F | p-value |
| Gender effect in experimental group | 1 | 5.05 | 4.33 | 0.050 |
| Gender effect in control group | 1 | 1.42 | 1.22 | 0.284 |
As it can be inferred from the above table, the effect of gender was significant on the experimental group at p=0.05. This means that the gender showed significant differences in general anxiety (GAD) only in the experimental group. Furthermore, the group therapy with CBT approach typically results in anxiety reduction in females.
Discussion
The present study aimed at examining the effect of group therapy with CBT approach on anxiety, fasting blood sugar and hemoglobin “A1c”in patients with diabetic (type II). The experimental group members participated in group therapy sessions under the exact same conditions. The anxiety questionnaires were distributed before and after therapy sessions and the fasting blood sugar and hemoglobin “A1c”level were measured prior to and following the sessions. The same tests were also carried out on the control group who did not participate in group therapy. Participants’ blood samples were sent to the laboratory to be analyzed with auto analyzer and spectrophotometer tools. Age, gender and history of diabetes were considered as research control variables. Pre-test variable was considered as the covariate to control the possible effects on the results.
The analysis of co-variance was used in order to examine the main effects of gender and group and their interactional effect on dependent variables and variables under study including fasting blood sugar, glycosylated HbA1c, and general anxiety disorder (GAD-7). The results showed no significant difference between the main effects of the group for comparing fasting blood sugar between experimental and control groups, and also the main effect of the gender for comparing fasting blood sugar between males and females. However, regarding the low level of fasting blood sugar in experimental group in comparison to control group, it can be inferred that the low number of samples or other uncontrolled factors such as age could affect the results and render the differences insignificant.
The main effect of group membership was significant on the dependent variable of glycosylated hemoglobin for comparing the concentration changes between the experimental and control groups. This result confirmed the positive effect of group therapy on lowering the glycosylated hemoglobin A1c. On the other hand, the main effect of group membership for comparing the level of anxiety (SAS) between the experimental and control group, and also the main effect of gender for comparing the level of anxiety between males and females showed no significant difference. The interactional effect of group by gender for comparing the level of general anxiety (GAD) in the control and experimental groups indicated significant difference. After repeating the analysis (with MANOVA method), the simple effects of group and gender were computed and the results revealed that the gender in experimental group showed significant differences in general anxiety. Regarding the lower mean of anxiety in females, it can be inferred that the group therapy with CBT approach is more effective for females.
To discuss the findings of the study, it should be considered that most of emotional problems such as anxiety are due to the individual’s communication problems, ensuing isolation, exclusion, inability to interact purposefully with others and loneliness. Although the therapist could help the individual to solve some of these problems, the main issue is whether or not the patient is able to implement the attitudes and strategies he/she has learned through the therapy sessions in his daily life or not. During group therapy sessions, the patient can solve his or her problems in front of others and understand others reactions and feedbacks. CBT approach is based on the idea that there exists an association among the individual’s thoughts, actions and moods. In this method, the patient’s interpretation of disease symptoms is emphasized rather than the disease symptoms themselves.
In cognitive behavior therapy, the main purpose is to determine and change negative thoughts related to depression and anxiety, and to focus on positive thoughts. The reduction of hemoglobin A1c after the three months of group therapy indicates that the lack of knowledge regarding the therapeutic triangle can increase the blood sugar. After the participation of patients in group therapy and their awareness as to how to control their diets, exercise, confront their negative thoughts and correct their interpretation of the diabetes symptoms, we observed a reduction in the level of glycosylated hemoglobin in both genders.
Previous studies [4,8,9,11,13] were carried out on diabetes “type I”, adolescent diabetes, or diabetes of both types ' I ' and ' II '. The present study aimed at patients with diabetic mellitus ' type II '. The results of this study confirmed that of many previous studies mentioned in the literature review regarding the reduction of anxiety [4,9]. This study is based on socio-psychological interventions with cognitive behavioral approach.
In the studies carried out on diabetes “type I”, the glycosylated hemoglobin did not decrease after the group therapy. For instance, Rossello and Bernhal [10] studied on a number of diabetic patients of type (I). They reached the same results except that the absence of a control group is one of the most important shortcomings of their study.
In this study, using covariance analysis, we patently observed the reduction of A1C hemoglobin in type (II) diabetic patients. On the other hand, the reduction in fasting blood sugar level was also notice able given the observed power (ή2=0.343) and the low mean of fasting blood sugar in comparison with control group.
According to a comprehensive study [20] (including 27 research studies), the prevalence of anxiety disorder symptoms is higher in females than in males; the same finding goes for diabetes type (I) and (II). This study was carried out on 4076 diabetic patients, and according to the findings, 55.3% of females and 32.9% of males suffered from anxiety disorders. General anxiety disorder (GAD) had the most prevalence (40%) [20]. Factors resulting in anxiety in females can be mostly related to their lack of awareness of disease symptoms, wrong interpretation of the symptoms and unreasonable and excessive attention to physical symptoms. In this study, we found out that the group therapy with the cognitive behavioral approach was more conducive to anxiety reduction in females compared to males which can be owing to the social engagement and interaction of the female members of the group.
The participants of the study were selected from the patients referred to a Para clinical center, which might have increased their level of anxiety. The low number of the study samples also limited the generalization of the results, hence the necessity of more studies with a higher number of samples. All patients, as a rule, used blood glucose lowering drugs, but only insulin was considered in this study and another drug was not evaluated. It was better to check the amount of blood glucose 2 hours after meals in addition to FBS. We suggest that future studies consider the variable of blood glucose 2 hours after food for statistical analyses. Moreover, since this is a practical kind of study, financial problems may be encountered by researchers; therefore, it is only logical to consider the pecuniary aspect in future studies.
As there was no significant difference between the experimental and control group as far as the reduction of blood sugar mean, it is suggested that future studies be carried out with more participants and with the omission of control factors such as age. More studies should be performed regarding the observed effect of cognitive behavioral method in the reduction of glycosylated hemoglobin in type (II) and type (I) diabetic patients. It is also recommended that the anxiety disorder records of diabetic patients be kept in hospitals. The internal medicine specialists or general practitioners could refer such patients to psychological services centers. Diabetes society centers should provide psychological supports and services and through, for instance, holding monthly sessions. We also propose that special centers be constructed for doing wider research on anxiety conditions.
Conclusion
In conclusion, our study shows that group cognitive-behavior therapy is an effective non pharmacologic treatment for anxiety symptoms in patients with type II diabetes. This therapy was associated with improvement in HbA1c despite the ineffectiveness of this intervention on reducing fasting blood glucose.
Acknowledgments
The authors would like to thank Dr. Kamran Gholamin, the head of the laboratory of medical diagnosis for his editorial assistance.
Conflict of Interest
The authors have no conflicts of interest.
References
Discussion
The present study aimed at examining the effect of group therapy with CBT approach on anxiety, fasting blood sugar and hemoglobin “A1c”in patients with diabetic (type II). The experimental group members participated in group therapy sessions under the exact same conditions. The anxiety questionnaires were distributed before and after therapy sessions and the fasting blood sugar and hemoglobin “A1c”level were measured prior to and following the sessions. The same tests were also carried out on the control group who did not participate in group therapy. Participants’ blood samples were sent to the laboratory to be analyzed with auto analyzer and spectrophotometer tools. Age, gender and history of diabetes were considered as research control variables. Pre-test variable was considered as the covariate to control the possible effects on the results.
The analysis of co-variance was used in order to examine the main effects of gender and group and their interactional effect on dependent variables and variables under study including fasting blood sugar, glycosylated HbA1c, and general anxiety disorder (GAD-7). The results showed no significant difference between the main effects of the group for comparing fasting blood sugar between experimental and control groups, and also the main effect of the gender for comparing fasting blood sugar between males and females. However, regarding the low level of fasting blood sugar in experimental group in comparison to control group, it can be inferred that the low number of samples or other uncontrolled factors such as age could affect the results and render the differences insignificant.
The main effect of group membership was significant on the dependent variable of glycosylated hemoglobin for comparing the concentration changes between the experimental and control groups. This result confirmed the positive effect of group therapy on lowering the glycosylated hemoglobin A1c. On the other hand, the main effect of group membership for comparing the level of anxiety (SAS) between the experimental and control group, and also the main effect of gender for comparing the level of anxiety between males and females showed no significant difference. The interactional effect of group by gender for comparing the level of general anxiety (GAD) in the control and experimental groups indicated significant difference. After repeating the analysis (with MANOVA method), the simple effects of group and gender were computed and the results revealed that the gender in experimental group showed significant differences in general anxiety. Regarding the lower mean of anxiety in females, it can be inferred that the group therapy with CBT approach is more effective for females.
To discuss the findings of the study, it should be considered that most of emotional problems such as anxiety are due to the individual’s communication problems, ensuing isolation, exclusion, inability to interact purposefully with others and loneliness. Although the therapist could help the individual to solve some of these problems, the main issue is whether or not the patient is able to implement the attitudes and strategies he/she has learned through the therapy sessions in his daily life or not. During group therapy sessions, the patient can solve his or her problems in front of others and understand others reactions and feedbacks. CBT approach is based on the idea that there exists an association among the individual’s thoughts, actions and moods. In this method, the patient’s interpretation of disease symptoms is emphasized rather than the disease symptoms themselves.
In cognitive behavior therapy, the main purpose is to determine and change negative thoughts related to depression and anxiety, and to focus on positive thoughts. The reduction of hemoglobin A1c after the three months of group therapy indicates that the lack of knowledge regarding the therapeutic triangle can increase the blood sugar. After the participation of patients in group therapy and their awareness as to how to control their diets, exercise, confront their negative thoughts and correct their interpretation of the diabetes symptoms, we observed a reduction in the level of glycosylated hemoglobin in both genders.
Previous studies [4,8,9,11,13] were carried out on diabetes “type I”, adolescent diabetes, or diabetes of both types ' I ' and ' II '. The present study aimed at patients with diabetic mellitus ' type II '. The results of this study confirmed that of many previous studies mentioned in the literature review regarding the reduction of anxiety [4,9]. This study is based on socio-psychological interventions with cognitive behavioral approach.
In the studies carried out on diabetes “type I”, the glycosylated hemoglobin did not decrease after the group therapy. For instance, Rossello and Bernhal [10] studied on a number of diabetic patients of type (I). They reached the same results except that the absence of a control group is one of the most important shortcomings of their study.
In this study, using covariance analysis, we patently observed the reduction of A1C hemoglobin in type (II) diabetic patients. On the other hand, the reduction in fasting blood sugar level was also notice able given the observed power (ή2=0.343) and the low mean of fasting blood sugar in comparison with control group.
According to a comprehensive study [20] (including 27 research studies), the prevalence of anxiety disorder symptoms is higher in females than in males; the same finding goes for diabetes type (I) and (II). This study was carried out on 4076 diabetic patients, and according to the findings, 55.3% of females and 32.9% of males suffered from anxiety disorders. General anxiety disorder (GAD) had the most prevalence (40%) [20]. Factors resulting in anxiety in females can be mostly related to their lack of awareness of disease symptoms, wrong interpretation of the symptoms and unreasonable and excessive attention to physical symptoms. In this study, we found out that the group therapy with the cognitive behavioral approach was more conducive to anxiety reduction in females compared to males which can be owing to the social engagement and interaction of the female members of the group.
The participants of the study were selected from the patients referred to a Para clinical center, which might have increased their level of anxiety. The low number of the study samples also limited the generalization of the results, hence the necessity of more studies with a higher number of samples. All patients, as a rule, used blood glucose lowering drugs, but only insulin was considered in this study and another drug was not evaluated. It was better to check the amount of blood glucose 2 hours after meals in addition to FBS. We suggest that future studies consider the variable of blood glucose 2 hours after food for statistical analyses. Moreover, since this is a practical kind of study, financial problems may be encountered by researchers; therefore, it is only logical to consider the pecuniary aspect in future studies.
As there was no significant difference between the experimental and control group as far as the reduction of blood sugar mean, it is suggested that future studies be carried out with more participants and with the omission of control factors such as age. More studies should be performed regarding the observed effect of cognitive behavioral method in the reduction of glycosylated hemoglobin in type (II) and type (I) diabetic patients. It is also recommended that the anxiety disorder records of diabetic patients be kept in hospitals. The internal medicine specialists or general practitioners could refer such patients to psychological services centers. Diabetes society centers should provide psychological supports and services and through, for instance, holding monthly sessions. We also propose that special centers be constructed for doing wider research on anxiety conditions.
Conclusion
In conclusion, our study shows that group cognitive-behavior therapy is an effective non pharmacologic treatment for anxiety symptoms in patients with type II diabetes. This therapy was associated with improvement in HbA1c despite the ineffectiveness of this intervention on reducing fasting blood glucose.
Acknowledgments
The authors would like to thank Dr. Kamran Gholamin, the head of the laboratory of medical diagnosis for his editorial assistance.
Conflict of Interest
The authors have no conflicts of interest.
References
- Lipowski ZJ. Psychosomatic Medicine and Liaison Psychiatry. Springer Science + Business Media; 1985; doi.org/10.1007/978-1-4613-2509-3
- Green SA. Psychological Factors Affecting Medical Conditions. Gen Hosp Psychiatry 1997; 19(2):158-9. doi.org/10.1016/s0163-8343(96)00157-0
- Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The Prevalence of Comorbid Depression in Adults with Diabetes a Meta-analysis. Diabetes care 2001; 24(6):1069-78.doi.org/10.2337/diacare.24.6.1069
- Lustman PJ, Griffith LS, Freedland KE, Kissel SS, Clouse RE. Cognitive Behavior Therapy for Depression in Type 2 Diabetes Mellitus: A Randomized, Controlled Trial. Ann Intern Med 1998; 129(8):613-21.doi.org/10.7326/0003-4819-129-8-199810150-00005
- Huang C-J, Chiu H-C, Lee M-H, Wang S-Y. Prevalence and Incidence of Anxiety Disorders in Diabetic Patients: a National Population-based Cohort Study. Gen Hosp Psychiatry 2011; 33(1):8-15. doi.org/10.1016/j.genhosppsych.2010.10.008
- Peyrot MF, McMurry JF. Stress Buffering and Glycemic Control: The Role of Coping Styles. Diabetes Care 1992; 15(7):842-6. doi.org/10.2337/diacare.15.7.842
- Regier DA. One-Month Prevalence of Mental Disorders in the United States. Arch Gen Psychiatry 1988; 45(11):977. doi. org/10.1001/archpsyc.1988.01800350011002
- Derakhshanpoor F, Farsinia M, Shahini N. Evaluation of Relation Between Anxiety Disorders with Diabetic Type Two Patients's Quality of Life Reffering to Gorgan's 5th Azar Clinic of Diabetes in 2012. Eur Psychiatry 2015; 30:482. doi.org/10.1016/s0924-9338(15)30379-5
- Delamater AM, Jacobson AM, Anderson B, Cox D, Fisher L, Lustman P, et al. Psychosocial Therapies in Diabetes: Report of the Psychosocial Therapies Working Group. Diabetes Care 2001; 24(7):1286-92. doi.org/10.2337/diacare.24.7.1286
- Silva RR, Gallagher R, Minami H. Cognitive-behavioral Treatments for Anxiety Disorders in Children and Adolescents. Prim Psychiatry 2006; 13(5):68.
- Camara A, Baldé NM, Enoru S, Bangoura JS, Sobngwi E, Bonnet F. Prevalence of Anxiety and Depression among Diabetic African Patients in Guinea: Association with HbA1c Levels. Diabetes Metab 2015; 41(1):62–8. doi.org/10.1016/j.diabet.2014.04.007
- Ironson G, Fitch C. Mental Health, Medical Illness, and Treatment with a Focus on Depression and Anxiety. Encyclopedia of Mental Health (Second Edition). 2016; 107–18. doi.org/10.1016/b978-0-12-397045-9.00135-x
- Evans G, Lewin TJ, Bowen K, Lowe J. Dealing with Anxiety: A Pilot Cognitive Behavioural Therapy Program for Diabetic Clinic Outpatient Attendees. International Journal of Diabetes Mellitus 2010; 2(1):51-5. doi.org/10.1016/j.ijdm.2009.12.010
- Roth A, Fanagony P. What Workers for Whom: A Critical Review of Psychotherapy Research. 2nd ed. London: The Guilford Press; 2005.
- Cohen J. Statistical Power Analysis for the Behavioral Sciences Lawrence Earlbaum Associates. Hillsdale, NJ. 1988.
- Zung WW. A Rating Instrument for Anxiety Disorders. Psychosomatics. 1971;12(6):371-9.
- Zung W. How Normal Is Anxiety? Current Concepts. Upjohn, Durham; 1980.
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A Brief Measure for Assessing Generalized Anxiety Disorder: the GAD-7. Arch Intern Med 2006; 166(10): 1092-7. doi.10.1001/archinte.166.10.1092
- Kendall PC, Hudson JL, Gosch E, Flannery-Schroeder E, Suveg C. Cognitive-behavioral Therapy for Anxiety Disordered Youth: A Randomized Clinical Trial Evaluating Child and Family Modalities. J Consult Clin Psychol 2008;76(2):282. doi.10.1037/0022-006X.76.2.282.
- Grigsby AB, Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. Prevalence of Anxiety in Adults with Diabetes: A Systematic Review. J Psychosom Res 2002; 53(6):1053-60.doi.org/10.1016/s0022-3999(02)00417-8
Type of Study: Research |
Subject:
Special
Received: 2017/08/7 | Accepted: 2017/08/7 | Published: 2017/08/7
Received: 2017/08/7 | Accepted: 2017/08/7 | Published: 2017/08/7
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information
Caspian Journal of Neurological Sciences
Guilan University of Medical Sciences
University Tel : +9813 3333 0939
E-mail: cjnsgums@gmail.com, cjns@gums.ac.ir
